Is size that important?
I think it is..otherwise why and my mom would discuss every time when they meet about my size that is expected I am born!
When mom started searching the net there were so many information available about new born size and how they should weigh when they come out on their mom's lap..
The newborn size:
In their first year, newborns grow a big way, with most tripling their birth weight and increasing their length by about 50%.
From your baby's first day, health care providers will keep track of weight, length, and head size. Growth is a good indicator of general health, and babies who are progressing well are generally healthy, while poor growth can be a sign of a problem.
What Newborns Weigh
Just like adults, newborns come in a range of healthy sizes. Most full-term babies (born between 37 and 40 weeks) weigh somewhere between 6 pounds, 2 ounces (2,812 grams) and 9 pounds, 2 ounces (4,173 grams). Their average length ranges from 19 to 21 inches (48 to 53 centimeters).
A newborn who is lighter or heavier than the average range is probably perfectly fine but might receive extra attention from the doctors and nurses after delivery just to make sure there are no problems.
A number of things can affect a baby's size at birth. The length of the pregnancy is important. Babies born at their due date or later tend to be larger than those born earlier. Babies born prematurely are often smaller than full-term babies.
Other factors include:
* Size of parents. Tall parents may have larger-than-average newborns; short parents may have smaller-than-average newborns.
* Multiple births. If you're having twins, triplets, or more, you can count on your babies being relatively small. Multiples not only have to share their growing space in the uterus, they also are often born early, which leads to small size at birth.
* Birth order. First babies are sometimes smaller than brothers or sisters born later.
* Gender. Girls tend to be smaller, boys larger, but the differences are slight at birth.
* Mother's health during pregnancy. Factors that can lead to a lower birth weight include a mother's high blood pressure, heart problems, or use of cigarettes, alcohol, or illegal drugs during the pregnancy. If the mother has diabetes, the baby may have a higher birth weight. All conditions that can affect a baby's weight should be closely monitored by the mother's doctor. In addition, women should not smoke, drink alcohol, or use illegal drugs during pregnancy.
* Nutrition during pregnancy. Proper nutrition is essential for a baby's growth in the uterus and beyond. A poor diet during pregnancy can affect how much a newborn weighs and how the infant grows.
* Baby's health. Medical problems, including some birth defects and certain infections acquired during the pregnancy, can affect a child's birth weight and later growth.
Growth and Premature Babies
Premature babies generally are smaller and lighter than other newborns. A preemie's weight will be largely determined by how early he or she was born. The time the infant has missed being in the womb was growing time, so the baby has to do that growing in the outside world.
Many pre-term babies are classified as having "low birth weight" or "very low birth weight." In medical terms, "low birth weight" means a baby weighs less than 5 pounds, 8 ounces (2,630 grams) at birth. That's the case for about 1 in every 13 babies in the United States, so it's quite common. "Very low birth weight" means a baby weighs less than 3 pounds, 5 ounces (1,587 grams). Most babies with low or very low birth weight were born prematurely.
Premature babies are given special medical attention immediately after birth, and a pediatric specialist called a neonatologist may be involved in their care. Many premature babies spend time in the neonatal intensive care unit (NICU) while they receive medical care, including feeding and observation of growth.
Is Bigger Better?
In the old days, a "strapping" baby with chubby cheeks and dimpled thighs was many people's picture of a healthy newborn. But a baby born much larger than average may have special medical problems that need attention. Some exceptionally large babies, especially those born to mothers with diabetes, including gestational diabetes, may have problems for a few days keeping blood sugar levels up and may require extra feedings, or even intravenous glucose, to prevent those levels from falling too low.
How Newborns Grow
Babies are born with some extra fluid, so it is perfectly normal for a newborn to drop a few ounces when that fluid is lost in the first few days of life. A healthy newborn is expected to lose 7% to 10% of the birth weight but should regain that weight by about 2 weeks after birth.
During their first month, most newborns continue to gain weight at a rate of at least 5 ounces (141 grams) a week. They generally grow in height about 1 to 1.5 inches (2.54 to 3.81 centimeters) during the first month. Many newborns go through a period of rapid growth when they are 7 to 10 days old and again at 3 and 6 weeks.
Should I Be Concerned?
Newborns are so small, and it can be hard to know if your baby is gaining weight the way he or she should. You may worry that your baby has lost too much weight in the first few days or isn't taking enough breast milk or formula. Most likely, everything is fine. But if you are concerned at all, check with your doctor.
What's Next?
Being small or large at birth doesn't necessarily mean a baby will be small or large later in childhood or as an adult. Plenty of towering teenagers began life as small babies, and the biggest baby on the block can grow up to be a petite adult.
By the time they're adults, kids tend to resemble their parents in size. Genetics, as well as good nutrition and your attention, will play a large part in determining how your baby grows in the years to come.
Whether your baby starts out large, small, or in between, in the next few months you can expect your infant to keep growing fast.
http://kidshealth.org/parent/growth/
The Normal Newborn
The average duration of pregnancy is 40 weeks. A baby born after this period weighs 2.8 kg. ( on an average ).
Any newborn with a birth weight of < 2.5 kg. is classified as a Low Birth Weight Baby and needs special care.
Following are the characteristics of a normal newborn baby:
* Weight 2.5 – 3.5 kg.
* Length 50 cm.
* Head circumference 35 cm.
* Heart rate 120 – 140 per minute.
* Respiratory rates 30 – 40 per minute.
The normal baby may be slightly bluish in the extremities a short while after birth but becomes pink within a few hours.
Urine is passed during birth or immediately after birth, but a vast majority passes urine within the 24 hours.
The first stool, which the baby passes, is known as meconium, it is black in color and is paste like. Meconium is passes within the first day and the stools change to golden brown over the next 2 – 3 days.
The infant is normally ready for the feed within 3 – 4 hours after birth and where ever possible should be put to the mother’s breast.
http://health.indiamart.com/kidshealth/newborn/
Friday, June 25, 2010
Monday, June 21, 2010
Baby's position:
Nowadays mom worry a lot about my position. She tries to find out how I am lying inside her. But mum you need to understand that I love playing here all the time..I also donot understand which side is top and which is bottom..
I have heard there are different orientations of a baby possible and depending on that they are named differently.
Normal Position Of The Baby
Normal Fetal Position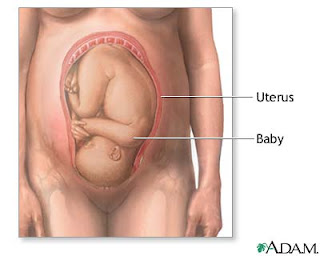 The term "fetal presentation" refers to the part of your baby's body that is closest to the birth canal. In most full-term pregnancies, the baby is positioned head down, or cephalic, in the uterus.
The term "fetal presentation" refers to the part of your baby's body that is closest to the birth canal. In most full-term pregnancies, the baby is positioned head down, or cephalic, in the uterus.
Breech Presentation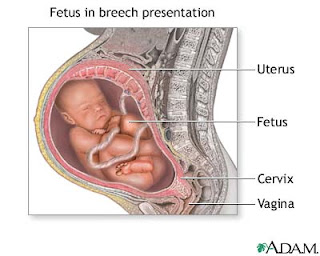 If your baby is breech, his bottom is the part of his body closest to the birth canal. No one is sure what causes a breech presentation, but it happens in 3% to 5% of single-baby deliveries.
If your baby is breech, his bottom is the part of his body closest to the birth canal. No one is sure what causes a breech presentation, but it happens in 3% to 5% of single-baby deliveries.
As your pregnancy nears full term, your caregiver will check your baby's position during regular prenatal visits. Common methods for assessing fetal position include vaginal exams, feeling your abdomen, and listening to the baby's heartbeat with a Doppler device.
Types Of Breech Presentation
 There are three types of breech presentation: complete, incomplete, and frank.
There are three types of breech presentation: complete, incomplete, and frank.
Complete breech is when both of the baby's knees are bent and his feet and bottom are closest to the birth canal.
Incomplete breech is when one of the baby's knees is bent and his foot and bottom are closest to the birth canal.
Frank breech is when the baby's legs are folded flat up against his head and his bottom is closest to the birth canal.
Complications of Breech
Prolapsed Umbilical Cord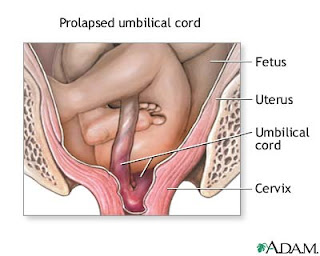 A prolapsed umbilical cord is common in breech deliveries. This happens when part of the umbilical cord slips down through the cervix before the baby does. The cord is then compressed during contractions, which cuts down on blood flow to the baby. An emergency cesarean section is usually needed.
A prolapsed umbilical cord is common in breech deliveries. This happens when part of the umbilical cord slips down through the cervix before the baby does. The cord is then compressed during contractions, which cuts down on blood flow to the baby. An emergency cesarean section is usually needed.
Correcting Breech
External Version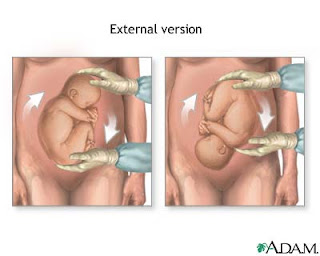 If you're near term and your baby is breech, your doctor may try to manually move him into a head-down position for delivery. There are two ways to do this: During an external version, the doctor moves your baby by pressing on the outside of your belly. During an internal version, the doctor inserts his hand through your vagina and cervix and moves the baby from the inside.
If you're near term and your baby is breech, your doctor may try to manually move him into a head-down position for delivery. There are two ways to do this: During an external version, the doctor moves your baby by pressing on the outside of your belly. During an internal version, the doctor inserts his hand through your vagina and cervix and moves the baby from the inside.
If your doctor can't manually reposition your baby, a cesarean section may be needed.
Other Presentations
Posterior Presentation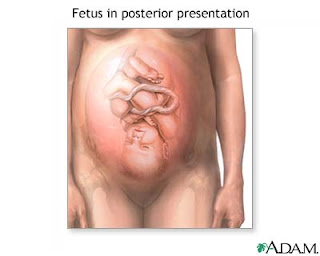 If your baby is in a posterior position, his face is turned up toward your belly. This can make labor longer and more difficult, since the widest part of his head has to fit through the birth canal.
If your baby is in a posterior position, his face is turned up toward your belly. This can make labor longer and more difficult, since the widest part of his head has to fit through the birth canal.
You may be able to help your baby rotate into a normal, face-down position by getting on all fours with your bottom in the air, which allows your uterus to drop forward. Your doctor may also try to reposition your baby by reaching in through your vagina and gently rotating his head with his hand or forceps. If none of these methods works, a cesarean section may be needed.
Other Presentations
Transverse Lie If your baby is transverse, he is lying horizontally in your uterus. Your doctor may try to manually turn him into a head-down position, but a cesarean section is usually needed.
If your baby is transverse, he is lying horizontally in your uterus. Your doctor may try to manually turn him into a head-down position, but a cesarean section is usually needed.
http://www.pennmedicine.org/health_info/
I have heard there are different orientations of a baby possible and depending on that they are named differently.
Normal Position Of The Baby
Normal Fetal Position
 The term "fetal presentation" refers to the part of your baby's body that is closest to the birth canal. In most full-term pregnancies, the baby is positioned head down, or cephalic, in the uterus.
The term "fetal presentation" refers to the part of your baby's body that is closest to the birth canal. In most full-term pregnancies, the baby is positioned head down, or cephalic, in the uterus.Breech Presentation
 If your baby is breech, his bottom is the part of his body closest to the birth canal. No one is sure what causes a breech presentation, but it happens in 3% to 5% of single-baby deliveries.
If your baby is breech, his bottom is the part of his body closest to the birth canal. No one is sure what causes a breech presentation, but it happens in 3% to 5% of single-baby deliveries.As your pregnancy nears full term, your caregiver will check your baby's position during regular prenatal visits. Common methods for assessing fetal position include vaginal exams, feeling your abdomen, and listening to the baby's heartbeat with a Doppler device.
Types Of Breech Presentation
 There are three types of breech presentation: complete, incomplete, and frank.
There are three types of breech presentation: complete, incomplete, and frank.Complete breech is when both of the baby's knees are bent and his feet and bottom are closest to the birth canal.
Incomplete breech is when one of the baby's knees is bent and his foot and bottom are closest to the birth canal.
Frank breech is when the baby's legs are folded flat up against his head and his bottom is closest to the birth canal.
Complications of Breech
Prolapsed Umbilical Cord
 A prolapsed umbilical cord is common in breech deliveries. This happens when part of the umbilical cord slips down through the cervix before the baby does. The cord is then compressed during contractions, which cuts down on blood flow to the baby. An emergency cesarean section is usually needed.
A prolapsed umbilical cord is common in breech deliveries. This happens when part of the umbilical cord slips down through the cervix before the baby does. The cord is then compressed during contractions, which cuts down on blood flow to the baby. An emergency cesarean section is usually needed.Correcting Breech
External Version
 If you're near term and your baby is breech, your doctor may try to manually move him into a head-down position for delivery. There are two ways to do this: During an external version, the doctor moves your baby by pressing on the outside of your belly. During an internal version, the doctor inserts his hand through your vagina and cervix and moves the baby from the inside.
If you're near term and your baby is breech, your doctor may try to manually move him into a head-down position for delivery. There are two ways to do this: During an external version, the doctor moves your baby by pressing on the outside of your belly. During an internal version, the doctor inserts his hand through your vagina and cervix and moves the baby from the inside.If your doctor can't manually reposition your baby, a cesarean section may be needed.
Other Presentations
Posterior Presentation
 If your baby is in a posterior position, his face is turned up toward your belly. This can make labor longer and more difficult, since the widest part of his head has to fit through the birth canal.
If your baby is in a posterior position, his face is turned up toward your belly. This can make labor longer and more difficult, since the widest part of his head has to fit through the birth canal.You may be able to help your baby rotate into a normal, face-down position by getting on all fours with your bottom in the air, which allows your uterus to drop forward. Your doctor may also try to reposition your baby by reaching in through your vagina and gently rotating his head with his hand or forceps. If none of these methods works, a cesarean section may be needed.
Other Presentations
Transverse Lie
http://www.pennmedicine.org/health_info/
Fetal Development: 32 weeks

Nowadays I can hear almost all sounds and noises outside my mom's belly..
I can feel the rays of sunlight when mum goes to her balcony and stands there ..she does not no how much I love that time..its so dark in here :(
I want to come out fast..i really do not like to stay all these ten months waiting and contemplating about different things..
Even when my pappa calls me from outside and touches me I feel so exited and want to come out at the very moment itself and play with him..he also gets same excited when he sees my head bulging out from my mom's belly..he acts like a child! and continues to speak to me in gibberish..so silly..hee hee!
I have gained alot of weight in the past few days..and gradually mom is becoming a little relaxed by this. Actuallu due to the fact of diabetes and diet etc she was not gaining weight to that extent in the past few weeks. My grand mom was worried herself and tried to convey her anxiety to mom..now she is also happy..
Grand mom ..wait ..still a lot of weight gain is still pending on my side..
Your Baby - 32 Weeks Pregnant
Pregnancy Week 32 Your baby sleeps approximately 90 to 95 percent of the day now. His skin has become thicker and he continues to become more of a pinkish color. Your baby's movements will peak this week. From now on they will change in quantity and quality. Most of the wrinkles are disappearing from your baby's face, and there may be a lot of hair on his head. The weight gain has been fairly incredible
recently. Your baby is now almost 4 pounds and is 17 inches long.
Your Body
Pregnancy Week 32 The discomforts of pregnancy may be wearing you down. Remember to rest as much as you can. There are many things you can do to help relieve some of these discomforts such as massage, relaxation techniques, stretching, exercise, proper posture and a healthy, balanced diet. Be sure not to take any sort of pain medication - even over the counter remedies such as Tylenol or Advil - without first discussing it with your doctor.
You may be wondering about what the birthing process will truly be like. Depending upon whom you ask, you may find yourself with varying examples. According to reports and research, approximately ten percent of women will report that labor is truly painful, while another ten percent will report no pain at all. Everyone else is somewhere in the middle of this spectrum. Your experience will differ from others as you may have a different pain threshold, and may choose to use or not to use any type of medications during birth. There are many factors that can affect the amount of pain you will experience during birth.
Your body is producing a hormone called relaxin. This hormone is responsible for loosening or relaxing the pelvis, making it more mobile during delivery. You may feel the effects of this hormone in your legs as you experience waddling. Don't worry; this is only temporary. And when it comes time to give birth, you will be very grateful it's there.
Your fundus is approximately four inches above your navel.
Common Pregnancy Symptoms in Week 32
- Breast Changes: tenderness, fullness, darkening of the areola
- Frequent Urination
- Constipation
- Heartburn or Indigestion
- Headaches
- Marks
- Itching
- Round Ligament Pain
- Hemorrhoids
Monday, June 14, 2010
Fetal Development: 31 weeks

Yay! I am 31 weeks ..Hoorray..
Do you understand what that means?
Now the countdown of weeks left can be done in one digit..Both me and mom are happy..
Your Baby's Development This Week
Your baby is probably around 15-16 inches in length and weighs in around 3-4 pounds.
That fat layer is still building up, and with it the skin tone will continue to become more pink and less transparent in appearance.
The brain is becoming more ridged and grooved and the nerves are growing at a tremendous rate. Already the baby is processing information gleaned from all five senses.
Feel like the baby is doing a little dance in response to music? Might not be so much a funny image as a reality. Research has shown that babies do move in rhythm and response to musical input.
Pregnancy Symptoms You May Feel During Week 31
Have you noticed a sticky yellowish substance leaking from your breasts? The presence or absence of it is perfectly normal. Some women will leak this first stage of milk in the weeks before birth, others will only notice it after baby's arrival.
Other leaking issues? You might find it embarrassing, but many expectant moms experience urine leakage when sneezing, or maybe laughing. Wearing a pantyliner may help. Kegel exercises will be helpful as well.
Another uncomfortable reality? Your internal organs are not quite where they used to be. Your bladder feels squished, your lungs stuffed up higher into your chest and the uterus is a whole four inches above the belly button now.
You may experience a feeling of not being able to get your breath, but rest assured baby is breathing just fine. To help you breathe easier, try to sit and stand up straight, and sleep on your side, propped on pillows.
Visit With the Obstetrician
Sometime after 28 weeks your physician may order a Fetal Nonstress Test. This is a simple noninvasive procedure done in around thirty minutes time. Two belts will be placed on mother's abdomen, one to measure fetal heart rate, the other to monitor contractions. The baby's heart rate should increase with fetal activity, and should decrease at rest. Occasionally baby decides to nap during the test, and should that happen, sometimes a little buzzer will be used to wake up baby. This test may be ordered should there be any question on the level of fetal activity, or if there is a possibility of placental function issues, or if this is a high risk pregnancy.
Preparing for Baby
You and your partner may want to check into infant CPR and first aid classes now, as part of your preparation for the new arrival. It's a good idea for anyone who will be around baby, including grandparents or babysitters. The classes are often short and will bring a peace of mind to worrying new parents. Knowing that you are prepared for emergencies will make you feel much more confident as a new parent.
Pregnancy Lifestyle
Are you getting your body ready for labor? There are exercises that are helpful in preparing for childbirth. First of all, doing Kegel exercises daily will definitely help with labor and after wards. Contract those muscles you use to shut off the flow of urine. Work on holding for five seconds at a time, working up to 10 seconds contracted with 10 seconds rest in between. You should do three sets of 10 a day. Other exercises are yoga type stretches, that are geared to pregnant women and aid in strengthening and stretching and relaxing your muscles, especially those you'll rely on most during birth.
http://www.thebabycorner.com/pregnancy-calendar/
Fetal Development: 30 weeks

Though I am at present 31 weeks but still I have not told you what has happened when I was 30 weeks.
Hence have a look at the development status when fetus is 30 weeks and the mom is happy that she has reached the last leg of the journey :)
Your Baby:
Your baby now weighs almost 3 pounds - that like a head of a cabbage! And the length is about 17.7 inches.
The major development during this week is your baby's brain. Back then, the brain was just a smooth surface. Now it is characterized by grooves and indentations. This wrinkled appearance allows for the growth of the brain tissues. The bone marrow now begins to produce red blood cells.
The toenails are now beginning to grow.
Your baby's lanugo - which are the fine, downy hairs found in the body are starting to disappear. This is also the reason why premature babies have more lanugo than the full term ones.
Lanugo serves as a furry coat to protect your baby from extreme temperature. Since there are already baby fats and the brain can now function to regulate the body’s temperature, then there is no need for these hairs anymore. But a few can still be seen during childbirth.
Aside from the decreasing number of lanugo, the amniotic fluid also decreases in volume as the baby gets bigger- so she will need more space in the uterus to take up.
Your baby's eyesight continues to develop although it's not that clear yet. Even after birth, the baby can't see clearly until after two to three months. The vision then continnues to imporve throughout childhood. 29 weeks pregnant
, the baby's vision vision is still 20/400 out of the normal vision, which is 20/20.
Your body:
You may easily get tired and exhausted now that your baby weighs much heavier compared to the past months and especially if you have problems falling asleep.
Hormonal changes will make your ligaments more lax and the joints become looser. This is also in preparation for childbirth.
Another effect of the hormonal shifting is your mood swings. These may also be due to the uncomfortable symptoms that you are experiencing during the span of the pregnancy. These are just a normal part of pregnancy. But if you feel that the condition worsens from time to time and you can no longer handle it, then better consult your obstetrician or your psychologist, for you might be developing maternal depression.
You will still continue to have impaired circulation due to the fact that your growing uterus is continuing to put pressure on your veins and arteries.
The best position to allow better blood flow would be a left lying position when sleeping, which can aid in proper circulation to your organs and extremities.
The head of your baby is now putting pressure on your bladder, causing you to urinate more frequently. Your breast may become tender (again!) as they gear up for the production of milk.
You may notice that your heartburn is getting worse each week.
There are actually ways in which you can prevent heartburn like avoiding foods that are gastric irritants like spicy foods, fatty or fried foods, coffee, carbonated beverages, and also chocolates. Eat small yet frequent meals, and don't lie down while you are eating or right after a meal. Stress has also been associated with heartburn. So take time to relax and have frequent rest periods. You may also want to go to your health care provider if these things won't work.
http://www.easybabylife.com/
Betnosol Injection for lungs maturation:
What is this?
I am getting ready to inhale and exhale on my own in my mum's womb. But still why would any one prescribe my mum to take Betnosol injection for my lungs maturation?
I really do not understand what these doctors are upto these days!
My mom's gynecologist does not want to take any chances with my lungs maturation. I think she is also worried for the fact if I am born premature before 34 weeks..then what!
Hence to make my lungs in a workable condition she is prescribing mom to take the dose of 3ampules each for 2 consecutive days, 24 hours apart.
I am trying mom to let her know that mom I am lots of hiccups and practicing my best to make my small lungs ready for the world outside so that when I come out I can smell the fragrance of my mom's body and also gets the smell of the mouth watering kebabs and fish which my dad loves to eat and brings home sometimes.
But forget about the what if scenarios and we will have to prepare our shelves for the shots.
Mom get ready and read these info before we proceed..
Betnesol Injections during pregnancy:
Betnesol, or betamethasone, is administered during pregnancy when preterm birth is a possibility. The steroid injection helps to produce surfactant in the baby's lungs, allowing them to inflate without sticking together. Normally, babies do not make this surfactant on their own until much later in pregnancy, around 32-35 weeks. Getting steroid injections into the mother at least 24 hours prior to a premature birth improves the baby's ability to breathe, reducing ventilation time and possibly reducing NICU time.
If your doctors are recommending this injection for you, they should have detected something that tells them your baby is at risk for premature birth. While fibroids can put you at risk for miscarriage and preterm labor, a fetal fibronection test (FFN) can more conclusively tell if this pregnancy in particular is at risk. If you have not had a positive FFN test, and you are not currently having preterm labor or carrying multiples, then you should ask for documentation of why this shot is being recommended for you and what your alternatives are. Betamethasone is not without risks; it can be lifesaving for premature babies, but it can have consequences on learning and development down the road.
---------------
How does it work?
Betnesol injection contains the active ingredient betamethasone sodium phosphate, which is a type of medicine known as a corticosteroid. Corticosteroid medicines are derivatives of the corticosteroid hormones cortisol and aldosterone that are produced naturally by the adrenal glands. They are often simply called steroids, but it should be noted that they are very different from another group of steroids, called anabolic steroids, which have gained notoriety because of their abuse by some athletes and body builders.
Corticosteroids have many important functions on every organ system. They affect the strength of heart muscle and its response to natural chemicals affecting heart rate. They affect the water and salt balance in the body and also enable the body to cope with stress. Stress includes changes in temperature, pain, fear, anxiety and illness. Stress can be hazardous if the body is not equipped to cope due to low levels of corticosteroids.
Corticosteroids allow us to respond to stress by increasing the rate and force of the heartbeat, increasing blood supply to essential tissues (muscle, heart, brain), increasing the body's supply of energy by raising blood sugar and by several other effects on body systems.
If the body's natural level of steroid hormones is too low because the adrenal glands are not producing enough hormones (a condition called adrenal insufficiency, for example in Addison's disease or following surgical removal of the adrenal glands), this can cause various symptoms, such as dizziness, fatigue, weakness, gut symptoms, depression and joint and muscle pain. It can also lead to collapse and death if the body is put under stress. Low blood levels of corticosteroids must be treated with replacement therapy to allow the body to function normally. This is usually acheived with a combination of hydrocortisone and fludrocortisone tablets.
Betamethasone is given by injection in situations where the levels of corticosteroids in the body suddenly become too low, causing shock and collapse. This might be due to many reasons, including abnormal stress in people with Addison's disease. This is an emergency situation and Betnesol injection is used to provide rapid control of symptoms.
Corticosteroid hormones are also involved in controlling inflammatory responses in the body. Betamethasone has an anti-inflammatory effect and is used to decrease inflammation in various different diseases and conditions.
Betamethasone decreases inflammation by acting within cells to prevent the release of certain chemicals that are important in the immune system. These chemicals are normally involved in producing immune and allergic responses. By decreasing the release of these chemicals in a particular area, inflammation and allergic reactions are reduced. Betnesol injection is used in serious or emergency situations when rapid control of symptoms is needed, for example in severe asthma attacks or severe allergic reactions such as anaphylaxis.
Betamethasone can also be injected directly into inflamed soft tissue, for example in tennis elbow, to decrease inflammation in that particular area.
What is it used for?
* Severe allergic reactions, such as anaphylaxis, angioedema or severe asthma attack.
* Severe drop in blood pressure causing dizziness, paleness and sweating (shock) due to surgical or accidental trauma or severe infection.
* Inadequate production of natural steroid hormones by the adrenal glands (acute adrenal insufficiency) due to abnormal stress in people with Addison's disease, Simmond's disease, people who have had their adrenal glands surgically removed, and people with underactive adrenal glands due to prolonged corticosteroid therapy.
* Local injection into inflamed soft tissue, such as tennis elbow, tenosynovitis, or bursitis.
* Injection into the eye to reduce inflammation in the eye.
Warning!
* This medicine must not be stopped suddenly if you have been given more than 1mg daily for more than three weeks; if you have been given high doses (more than 6mg) even if only for three weeks or less; if you have been treated with corticosteroid tablets or injections in the last year; if you had problems with your adrenal glands before treatment was started; or if you have been given repeated doses in the evening. In these situations this medicine can suppress the natural production of corticosteroids by the adrenal glands, which means that the body becomes temporarily reliant on the medicine. When it is time to stop treatment the dose should be tapered down gradually, to allow the adrenal glands to start producing adequate amounts of natural steroids again. However, in general Betnesol injection is not intended for long-term use and is unlikely to be used for longer than two or three days. If corticosteroid treatment is still needed after this you are likely to be switched to a corticosteroid taken by mouth where possible. Other steroids should also not be stopped abruptly.
* If you are having long-term or repeated treatment with steroids you will be given a steroid card that you should carry with you at all times. Show it to anyone who treats you (eg doctor, nurse, pharmacist, dentist, anaesthetist). The card contains details of your prescriber, type of steroid, dose taken and the duration of treatment. It's purpose is to act as a reminder that your medicine should not be stopped suddenly, and to provide information of your treatment to other people treating you. This is important because the effects that corticosteroids have on the body may affect other medical treatment you may be given. If you have an accident the card contains information that could save your life. You should also show your steroid card to anyone who treats you for three months after you stop treatment with steroids.
* Corticosteroids decrease the body's natural immune and inflammatory responses. They may increase your susceptibility to infections and can also mask the symptoms of infections, making you think they are less serious than they are. For this reason, it is important to consult your doctor if you get any signs of infection during treatment.
* If you have never had chickenpox you could be at risk of severe chickenpox while having long-term treatment with this medicine and should avoid close personal contact with people who have chickenpox or shingles (herpes zoster). You should also avoid contact with people who have measles. If you are exposed to people with these diseases either during treatment, or in the three months after stopping treatment, you should consult your doctor urgently, as you will need an injection of immunoglobulin to help you stop getting the diseases. This is very important as these diseases can be life-threatening in people treated with long-term corticosteroids.
* Corticosteroid treatment, especially with high doses, can alter mood and behaviour early in treatment. People may experience confusion, irritability, nightmares, difficulty sleeping, mood changes and depression, and suffer from delusions and suicidal thoughts. In a few cases these effects have also occured when corticosteroid treatment is being withdrawn. For this reason, it is important to let your doctor know if you notice any change in your mood or behaviour during treatment or when stopping treatment, particularly if you begin to feel depressed, or have any disturbing thoughts or feelings. Most of these problems go away if the dose is lowered or the medicine is stopped. However if problems do happen they might need treatment.
* Children and adolescents having long-term treatment with this medicine should have their growth regularly monitored.
Use with caution in
* Children and adolescents.
* Elderly people.
* Decreased kidney function.
* Liver failure.
* Peptic ulcer.
* Inflammation of the bowel and back passage (ulcerative colitis).
* Painful inflammation of small sacs or pouches in the wall of the gut (diverticulitis).
* People who have recently had a surgical procedure called intestinal anastomosis, which involves the joining together of ends of the intestine after a section has been removed.
* People with a history of blood clots in the blood vessels (thromboembolism).
* Heart failure.
* People who have recently had a heart attack.
* High blood pressure (hypertension).
* Diabetes, or a family history of diabetes.
* Underactive thyroid gland (hypothyroidism).
* Epilepsy.
* Glaucoma, or a family history of glaucoma.
* Current severe psychiatric illness, or a personal or family history of psychiatric illness, including depression, manic depression or schizophrenia.
* History of psychiatric illness caused by the use of a corticosteroid.
* Osteoporosis.
* Women who have passed the menopause.
* Abnormal muscle weakness (myasthenia gravis).
* People who have previously experienced muscle disorders (myopathy) caused by steroids.
* People with a history of tuberculosis (TB).
* Herpes simplex virus infection of the eye.
* People with a low level of potassium in their blood (hypokalaemia).
Not to be used in
* People with widespread infection, unless this is being treated with specific anti-infectives.
* Corticosteroids should not be used for the management of head injury or stroke because they are unlikely to be of benefit and may even be harmful.
* Betnesol injection should not be injected directly into tendons.
This medicine should not be used if you are allergic to one or any of its ingredients. Please inform your doctor or pharmacist if you have previously experienced such an allergy.
If you feel you have experienced an allergic reaction, stop using this medicine and inform your doctor or pharmacist immediately.
Pregnancy and breastfeeding
Certain medicines should not be used during pregnancy or breastfeeding. However, other medicines may be safely used in pregnancy or breastfeeding providing the benefits to the mother outweigh the risks to the unborn baby. Always inform your doctor if you are pregnant or planning a pregnancy, before using any medicine.
* When administered for long periods or repeatedly during pregnancy, corticosteroids may increase the risk of slowed growth in the developing baby. They may also cause the baby to make less of its own steroid hormones after birth, but this usually resolves on its own and rarely causes any problems. When used during pregnancy betamethasone may also temporarily reduce the baby’s heart rate and body movements. As a result this medicine should be used with caution during pregnancy, and only if the expected benefit to the mother is greater than any possible risk to the developing baby. Seek further medical advice from your doctor.
* This medicine passes into breast milk. It should be used with caution in mothers who are breastfeeding and only if the benefits to the mother outweigh any risks to the nursing infant. Lower doses taken by the mother are unlikely to significantly affect the baby, but if the mother is taking high doses for long periods of time, the medicine could cause the baby's adrenal glands to make less of their own steroid hormones. Seek medical advice from your doctor.
Side effects
Medicines and their possible side effects can affect individual people in different ways. The following are some of the side effects that are known to be associated with this medicine. Just because a side effect is stated here does not mean that all people using this medicine will experience that or any side effect.
* Raised blood sugar level.
* Increased appetite and weight gain.
* Increased susceptibility to infections and increased severity of infections (see warnings above).
* Effects on the gut, such as indigestion or abdominal bloating, nausea, ulceration in the stomach or intestine, inflammation of the pancreas (pancreatitis).
* Ulceration or thrush infection in the throat.
* Muscle weakness or wasting.
* Thinning of the bones (osteoporosis) and increased risk of breaking a bone.
* Effects on the skin, such as skin thinning, impaired healing, acne, bruising, stretch marks, increased sweating, change in pigmentation, increased hair growth (hirsutism).
* Psychiatric reactions, such as mood changes (including irritability, depression and suicidal thoughts), psychotic reactions (including mania, delusions and hallucinations), anxiety, confusion, memory loss, sleep disturbances (see warning above).
* Cushing's syndrome, characterised by a moon face.
* Menstrual disturbances.
* Decrease in the production of natural steroids by the adrenal glands (adrenal suppression - see warning above).
* Effects on the eyes, such as raised pressure inside the eye (glaucoma), cataracts.
* Slowed growth in children and adolescents.
* Hiccups.
* Blood clots in the blood vessels (thromboembolism).
The side effects listed above may not include all of the side effects reported by the medicine's manufacturer.
For more information about any other possible risks associated with this medicine, please read the information provided with the medicine or consult your doctor or pharmacist.
How can this medicine affect other medicines?
It is important to tell your doctor or pharmacist what medicines you are already taking, including those bought without a prescription and herbal medicines, before you start treatment with this medicine. Similarly, check with your doctor or pharmacist before taking any new medicines while being treated with this one, to ensure that the combination is safe.
Betamethasone may increase blood sugar levels and so may oppose the blood sugar lowering effects of antidiabetic medicines. People with diabetes may need an increase in their dose of insulin or antidiabetic tablets.
Betamethasone may enhance the anti-blood-clotting effect of anticoagulant medicines such as warfarin. People taking anticoagulant medicines in combination with betamethasone should have their blood clotting time (INR) regularly monitored, particularly after starting or stopping treatment with betamethasone and after any dose changes.
If betamethasone is used in combination with non-steroidal anti-inflammatory drugs (NSAIDs) eg ibuprofen, there may be an increased risk of side effects on the gut, such as stomach ulceration and bleeding.
Betamethasone may decrease the blood levels of salicylates such as aspirin. When betamethasone is stopped, this may result in excessive levels of the salicylate, unless the dose is readjusted.
The following medicines may increase the removal of betamethasone from the body, thus reducing its effects. You may need a larger dose of betamethasone if you are also taking any of these medicines:
* barbituates, eg amobarbital, phenobarbital
* carbamazepine
* phenytoin
* primidone
* rifabutin
* rifampicin.
The effect of corticosteroids may be reduced in the three to four days following use of mifepristone.
The following medicines may reduce the removal of betamethasone from the body and so may increase its effects or side effects:
* ciclosporin (betamethasone may also increase the blood level and risk of side effects of ciclosporin)
* itraconazole
* ketoconazole
* macrolide-type antibiotics, eg erythromycin
* protease inhibitors, eg ritonavir.
Betamethasone may decrease the body's immune response. This means that vaccines may be less effective if given during treatment, because the body does not produce sufficient antibodies. Live vaccines may cause serious infections. Live vaccines include: measles, mumps, rubella, MMR, BCG, chickenpox, oral polio, oral typhoid and yellow fever. These should not be given to people whose immune system is underactive due to treatment with this medicine.
Corticosteroids can cause fluid and salt retention and so may oppose the effects of antihypertensive medicines used to treat high blood pressure, and diuretics such as furosemide. However, betamethasone is much less likely than other corticosteroids to have this effect.
Corticosteroids can also lower the amount of potassium in the blood, though this is much less likely with betamethasone than with other corticosteroids. However, there may be an increased chance of the level of potassium in the blood falling too low (hypokalaemia) if betamethasone is used in combination with the following medicines:
* acetazolamide
* amphotericin
* beta agonists, eg salbutamol, salmeterol, terbutaline
* carbenoxolone
* potassium-losing diuretics, eg furosemide, bendroflumethiazide
* theophylline.
Other medicines containing the same active ingredient
Betamethasone has many different uses and comes in many different forms. The factsheets below contain information about betamethasone used in various areas of the body.
-----------------------
Steroid Injection for Fetal Lung Development
Injections of corticosteroids for fetal lung development has been praised as one of the best advances in fetal medicine in the 90s. Since 1994 the National Institutes for Health and other professional organizations have encouraged their use in promoting the development of fetal lung development in moms who were at risk for preterm labor or birth.
Betamethasone and dexamethasone are the two most commonly used steroids. The average protocol was to give to intramuscular injections (IM) 24 hours apart. Some practitioners also choose to continually repeat the dosages every week until the birth. The injections had to be given 24-48 hours prior to the birth for maximum effect. They were also best used between weeks 24 and 34 gestation.
The use of the steroids provided benefits for the lung development in the premature infants to reduce the risk of respiratory distress syndrome (RDS) as well as to reduce the risk of intracranial hemorrhaging and some other potential benefits.
However, recent studies say that the benefits of multiple doses is questionable, particularly in light of potential risks. Citing the "limited quality" of the studies of multiple doses and the potential disadvantages the National Institute of Health issued a statement of August 18th that a single dose was sufficient in achieving the benefits desired.
Potential down sides to multiple doses can include: psychomotor delays, behavioral problems and the fact that the effects on neonatal mortality aren't known between the single and multiple dose courses. In separate findings by an Israeli study it was also noted that there is an increase in maternal infection with the use of steroids, so limiting doses may help with this side effect as well.
The steroid injection is to help mature the baby's lungs in case of premature delivery. Yes it has potential side effects (EVERY medication has potential side effects...there's no free ride when it comes to pharmacology). It develops the fetal lungs early because it sets up a very stressful environment for the baby. Decreased birth weight, decreased brain size, abnormal brain development, adverse effects on the fetal immune system, are just some of the potential side effects. Steroid injections for fetal lung development should not be taken lightly. It should be used only for cases where premature delivery is expected and the potential benefits outweigh the potential side effects.
I don't know why the doc told her that one injection is harmful but more than one is not. Sounds like she didn't really understand what was being explained to her.
http://www.naturallycurly.com/curltalk/showthread.php?t=27953
Antenatal corticosteroids for fetal lung development
Examples
betamethasone Celestone Soluspan dexamethasone Dalalone Decadron
How It Works
Betamethasone and dexamethasone cause an immature fetus's lungs to produce a compound called surfactant. A full-term baby's lungs naturally produce surfactant, which lubricates the lining of the air sacs within the lungs. This allows the inner surfaces of the air sacs to slide against one another without sticking during breathing. Premature infants whose lungs have begun producing surfactant have an improved ability to breathe on their own, or with less respiratory treatment, after birth.
When preterm birth between 24 and 34 weeks of pregnancy (gestation) is expected within 7 days, betamethasone or dexamethasone is given to the mother in order to affect the fetus. Betamethasone is given in 2 injections, 24 hours apart. Dexamethasone is given every 12 hours for 4 doses.
If delivery does not occur within 7 days of treatment, the injections should not be repeated. Recent guidelines issued by the National Institutes of Health discourage such repeat courses of treatment, based on concerns about fetal harm from repeat treatments.1
Why It Is Used
Corticosteroids are considered standard treatment for women who are 24 to 34 weeks pregnant and may deliver within the next 1 to 7 days, with or without preterm premature rupture of membranes (pPROM).1
Betamethasone and dexamethasone are corticosteroids, also called glucocorticoids, that are given before birth (antenatally) to speed up a preterm fetus's lung development. Either is used when a mother is in preterm labor and birth may occur in 24 to 48 hours. This helps prevent the occurrence of respiratory distress syndrome (RDS) and related complications following premature birth.
Many infants born at 33 to 34 weeks' gestation have sufficient lung maturity to breathe on their own. However, considering the low-risk, high-benefit nature of this treatment, corticosteroids are typically used up to 34 weeks of pregnancy.
WebMD
Betamethasone is often used in patients with premature labor at about 26-34 weeks' gestation to stimulate fetal lung maturation The benefits of this therapy are: Reduction in incidence of respiratory distress syndrome (RDS) Decreased severity of RDS if it occurs Decreased incidence of, and mortality from, intracranial hemorrhage Increased survival of premature infants Betamethasone crosses the placenta to the fetus . The drug is partially metabolized (47%) by the perfused placenta to its inactive 11-ketosteroid derivative, but less so than other corticosteroids, although the differences are not statistically significant .
In patients with premature rupture of the membranes (PROM), administration of betamethasone to the mother does not always reduce the frequency of RDS or perinatal mortality . An increased risk of maternal infection has also been observed in patients with PROM treated with corticosteroids . In a study comparing betamethasone therapy with nonsteroid management of women with PROM, neonatal sepsis was observed in 23% (5 of 22) of steroid-exposed newborns vs. only 2% (1 of 46) of the non-steroid-exposed group . A 1985 study also found increased neonatal sepsis in exposed newborns who were delivered more than 48 hours after PROM, 18.6% (14 of 75) vs. 7.4% (4 of 54) of nonexposed controls . In addition, moderate to severe respiratory morbidity was increased over that in controls, 21.3% vs. 11.1%, as well as overall mortality, 8% vs. 1.8% . Other reports, however, have noted beneficial effects of betamethasone administration to patients with PROM with no increase in infectious morbidity (15,23,24,). In women colonized with group B streptococci, the combined use of betamethasone and ampicillin improved the outcome of preterm pregnancies with PROM .
Betamethasone therapy is less effective in decreasing the incidence of RDS in male infants than in female infants . The reasons for this difference have not been discovered. Slower lung maturation in male fetuses has been cited as a major contributing factor to the sex differential noted in neonatal mortality. Therapy is also less effective in multiple pregnancies , even when doses have been doubled . In twins, only the first-born seems to benefit from antenatal steroid therapy .
An increased incidence of hypoglycemia in newborns exposed in utero to betamethasone has been reported . Other investigators have not observed this effect.
In the initial study examining the effect of betamethasone on RDS, investigators reported an increased risk of fetal death in patients with severe preeclampsia. They proposed that the corticosteroid had an adverse effect on placentas already damaged by vascular disease. A second study did not confirm these findings .
A case of suspected betamethasone-induced leukemoid reaction was observed in an 880-g, 30-weeks'-gestation female infant whose mother received 12 mg of betamethasone 4 hours prior to delivery . A second case, in a female infant born at 25-26 weeks' 71 hours after betamethasone, was published in 1997 . Within about 710 days, the white blood cell count had returned to normal in both infants. A 1984 study examined the effect of betamethasone on leukocyte counts in mothers with PROM or premature labor . No effect, as compared to untreated controls, was found in either group.
A case of acute, life-threatening exacerbation of muscular weakness requiring intubation and mechanical ventilation was reported in a 24-year-old woman who was treated with betamethasone, 12 mg IM, to enhance fetal lung maturity at 32 weeks' gestation . The onset of symptoms occurred 30 minutes after the corticosteroid dose. The authors attributed the crisis to betamethasone (adrenocorticosteroids are known to aggravate myasthenia) after other potential causes were ruled out. The infant was delivered by emergency cesarean section and, except for the typical problems related to prematurity, he had a normal hospital course.
Hypertensive crisis associated with the use of ritodrine and betamethasone has been reported . Systolic blood pressure was above 300 mm Hg with a diastolic pressure of 120 mm Hg. Although the hypertension was probably caused by ritodrine, it is not known whether the corticosteroid was a contributing factor.
Breast Feeding Summary
No reports describing the use of betamethasone during human lactation have been located. The molecular weight (about 435 for the acetate salt and about 517 for the sodium phosphate salt) are low enough, however, that excretion into milk should be expected.
http://drugsafetysite.com/betamethasone/
What should I watch for while taking betamethasone?
Visit your prescriber or health care professional for regular checks on your progress. If you are using corticosteroids for a long time, carry an identification card with your name, the type and dose of corticosteroid, and your prescriber's name and address. Do not suddenly stop using betamethasone. You may need to gradually reduce the dose, so that your body can adjust. Follow the advice of your prescriber or health care professional.
If you receive corticosteroids for a long time, avoid contact with people who have an infection. You may be at an increased risk from infection while receiving betamethasone. Tell your prescriber or health care professional if you are exposed to anyone with measles or chickenpox, or if you develop sores or blisters that do no heal properly.
People who are taking certain dosages of betamethasone may need to avoid immunization with certain vaccines or may need to have changes in their vaccination schedules to ensure adequate protection from certain diseases. Make sure to tell your prescriber or health care professional that you are taking betamethasone before receiving any vaccine.
If you are diabetic, betamethasone can affect your blood sugar levels. Check with your prescriber or health care professional if you need help adjusting the dose of your diabetic medicine.
If you are receiving betamethasone injections every day, you may need to watch your diet. Your body can also lose potassium while you receive this medicine. Ask your prescriber or health care professional about your diet, especially about your salt intake.
If you are going to have surgery tell your prescriber or health care professional that you are receiving betamethasone, or have taken it within the last 12 months.
If betamethasone has been injected into one of your joints, do not put too much stress on the joint for a while. Talk to your prescriber or health care professional about how much you can use the joint while it is healing.
Elderly patients have an increased risk of side effects from betamethasone.
Betamethasone can interfere with certain lab tests and can cause false skin test results.
What side effects may I notice from receiving betamethasone?
Side effects that you should report to your prescriber or health care professional as soon as possible:
• bloody or black, tarry stools
• confusion, excitement, restlessness, a false sense of well-being
• eye pain, decreased or blurred vision, or bulging eyes
• fever, sore throat, sneezing, cough, or other signs of infection
• frequent passing of urine
• hallucinations (seeing and hearing things that are not really there)
• increased thirst
• irregular heartbeat
• menstrual problems
• mental depression, mood swings, mistaken feelings of self-importance, mistaken feelings of being mistreated
• muscle cramps or muscle weakness
• nausea, vomiting
• pain in hips, back, ribs, arms, shoulders, or legs
• pain, redness, inflammation or scarring at the injection site
• rounding out of face
• skin problems, acne
• stomach pain
• swelling of feet or lower legs
• thin or shiny skin at the injection site
• unusual bruising or red pinpoint spots on the skin
• unusual tiredness or weakness
• weight gain or weight loss
• wounds that will not heal
Side effects that usually do not require medical attention (report to your prescriber or health care professional if they continue or are bothersome):
• headache
• increased appetite
• increased sweating
• nervousness, restlessness, or difficulty sleeping
• unusual increased growth of hair on the face or body
http://www.answers.com/topic/betamethasone-injection
Betamethasone is a corticosteroids, and as such can cause the following side effects:
Increased thirst and urination, lethargy, increased appetite, abortion during pregnancy, immune suppression (and thus more susceptible to other illnesses), muscle weakness and possible atrophy, stomach ulcers, diarrhea, panting, and possible bone weakness.
Now, keep in mind, these side effects are often rare, except for the increased drinking, urinating and eating. Also, these are much more likely to be seen in long term use, not one injection.
Read more: http://www.justanswer.com/questions/
I am getting ready to inhale and exhale on my own in my mum's womb. But still why would any one prescribe my mum to take Betnosol injection for my lungs maturation?
I really do not understand what these doctors are upto these days!
My mom's gynecologist does not want to take any chances with my lungs maturation. I think she is also worried for the fact if I am born premature before 34 weeks..then what!
Hence to make my lungs in a workable condition she is prescribing mom to take the dose of 3ampules each for 2 consecutive days, 24 hours apart.
I am trying mom to let her know that mom I am lots of hiccups and practicing my best to make my small lungs ready for the world outside so that when I come out I can smell the fragrance of my mom's body and also gets the smell of the mouth watering kebabs and fish which my dad loves to eat and brings home sometimes.
But forget about the what if scenarios and we will have to prepare our shelves for the shots.
Mom get ready and read these info before we proceed..
Betnesol Injections during pregnancy:
Betnesol, or betamethasone, is administered during pregnancy when preterm birth is a possibility. The steroid injection helps to produce surfactant in the baby's lungs, allowing them to inflate without sticking together. Normally, babies do not make this surfactant on their own until much later in pregnancy, around 32-35 weeks. Getting steroid injections into the mother at least 24 hours prior to a premature birth improves the baby's ability to breathe, reducing ventilation time and possibly reducing NICU time.
If your doctors are recommending this injection for you, they should have detected something that tells them your baby is at risk for premature birth. While fibroids can put you at risk for miscarriage and preterm labor, a fetal fibronection test (FFN) can more conclusively tell if this pregnancy in particular is at risk. If you have not had a positive FFN test, and you are not currently having preterm labor or carrying multiples, then you should ask for documentation of why this shot is being recommended for you and what your alternatives are. Betamethasone is not without risks; it can be lifesaving for premature babies, but it can have consequences on learning and development down the road.
---------------
How does it work?
Betnesol injection contains the active ingredient betamethasone sodium phosphate, which is a type of medicine known as a corticosteroid. Corticosteroid medicines are derivatives of the corticosteroid hormones cortisol and aldosterone that are produced naturally by the adrenal glands. They are often simply called steroids, but it should be noted that they are very different from another group of steroids, called anabolic steroids, which have gained notoriety because of their abuse by some athletes and body builders.
Corticosteroids have many important functions on every organ system. They affect the strength of heart muscle and its response to natural chemicals affecting heart rate. They affect the water and salt balance in the body and also enable the body to cope with stress. Stress includes changes in temperature, pain, fear, anxiety and illness. Stress can be hazardous if the body is not equipped to cope due to low levels of corticosteroids.
Corticosteroids allow us to respond to stress by increasing the rate and force of the heartbeat, increasing blood supply to essential tissues (muscle, heart, brain), increasing the body's supply of energy by raising blood sugar and by several other effects on body systems.
If the body's natural level of steroid hormones is too low because the adrenal glands are not producing enough hormones (a condition called adrenal insufficiency, for example in Addison's disease or following surgical removal of the adrenal glands), this can cause various symptoms, such as dizziness, fatigue, weakness, gut symptoms, depression and joint and muscle pain. It can also lead to collapse and death if the body is put under stress. Low blood levels of corticosteroids must be treated with replacement therapy to allow the body to function normally. This is usually acheived with a combination of hydrocortisone and fludrocortisone tablets.
Betamethasone is given by injection in situations where the levels of corticosteroids in the body suddenly become too low, causing shock and collapse. This might be due to many reasons, including abnormal stress in people with Addison's disease. This is an emergency situation and Betnesol injection is used to provide rapid control of symptoms.
Corticosteroid hormones are also involved in controlling inflammatory responses in the body. Betamethasone has an anti-inflammatory effect and is used to decrease inflammation in various different diseases and conditions.
Betamethasone decreases inflammation by acting within cells to prevent the release of certain chemicals that are important in the immune system. These chemicals are normally involved in producing immune and allergic responses. By decreasing the release of these chemicals in a particular area, inflammation and allergic reactions are reduced. Betnesol injection is used in serious or emergency situations when rapid control of symptoms is needed, for example in severe asthma attacks or severe allergic reactions such as anaphylaxis.
Betamethasone can also be injected directly into inflamed soft tissue, for example in tennis elbow, to decrease inflammation in that particular area.
What is it used for?
* Severe allergic reactions, such as anaphylaxis, angioedema or severe asthma attack.
* Severe drop in blood pressure causing dizziness, paleness and sweating (shock) due to surgical or accidental trauma or severe infection.
* Inadequate production of natural steroid hormones by the adrenal glands (acute adrenal insufficiency) due to abnormal stress in people with Addison's disease, Simmond's disease, people who have had their adrenal glands surgically removed, and people with underactive adrenal glands due to prolonged corticosteroid therapy.
* Local injection into inflamed soft tissue, such as tennis elbow, tenosynovitis, or bursitis.
* Injection into the eye to reduce inflammation in the eye.
Warning!
* This medicine must not be stopped suddenly if you have been given more than 1mg daily for more than three weeks; if you have been given high doses (more than 6mg) even if only for three weeks or less; if you have been treated with corticosteroid tablets or injections in the last year; if you had problems with your adrenal glands before treatment was started; or if you have been given repeated doses in the evening. In these situations this medicine can suppress the natural production of corticosteroids by the adrenal glands, which means that the body becomes temporarily reliant on the medicine. When it is time to stop treatment the dose should be tapered down gradually, to allow the adrenal glands to start producing adequate amounts of natural steroids again. However, in general Betnesol injection is not intended for long-term use and is unlikely to be used for longer than two or three days. If corticosteroid treatment is still needed after this you are likely to be switched to a corticosteroid taken by mouth where possible. Other steroids should also not be stopped abruptly.
* If you are having long-term or repeated treatment with steroids you will be given a steroid card that you should carry with you at all times. Show it to anyone who treats you (eg doctor, nurse, pharmacist, dentist, anaesthetist). The card contains details of your prescriber, type of steroid, dose taken and the duration of treatment. It's purpose is to act as a reminder that your medicine should not be stopped suddenly, and to provide information of your treatment to other people treating you. This is important because the effects that corticosteroids have on the body may affect other medical treatment you may be given. If you have an accident the card contains information that could save your life. You should also show your steroid card to anyone who treats you for three months after you stop treatment with steroids.
* Corticosteroids decrease the body's natural immune and inflammatory responses. They may increase your susceptibility to infections and can also mask the symptoms of infections, making you think they are less serious than they are. For this reason, it is important to consult your doctor if you get any signs of infection during treatment.
* If you have never had chickenpox you could be at risk of severe chickenpox while having long-term treatment with this medicine and should avoid close personal contact with people who have chickenpox or shingles (herpes zoster). You should also avoid contact with people who have measles. If you are exposed to people with these diseases either during treatment, or in the three months after stopping treatment, you should consult your doctor urgently, as you will need an injection of immunoglobulin to help you stop getting the diseases. This is very important as these diseases can be life-threatening in people treated with long-term corticosteroids.
* Corticosteroid treatment, especially with high doses, can alter mood and behaviour early in treatment. People may experience confusion, irritability, nightmares, difficulty sleeping, mood changes and depression, and suffer from delusions and suicidal thoughts. In a few cases these effects have also occured when corticosteroid treatment is being withdrawn. For this reason, it is important to let your doctor know if you notice any change in your mood or behaviour during treatment or when stopping treatment, particularly if you begin to feel depressed, or have any disturbing thoughts or feelings. Most of these problems go away if the dose is lowered or the medicine is stopped. However if problems do happen they might need treatment.
* Children and adolescents having long-term treatment with this medicine should have their growth regularly monitored.
Use with caution in
* Children and adolescents.
* Elderly people.
* Decreased kidney function.
* Liver failure.
* Peptic ulcer.
* Inflammation of the bowel and back passage (ulcerative colitis).
* Painful inflammation of small sacs or pouches in the wall of the gut (diverticulitis).
* People who have recently had a surgical procedure called intestinal anastomosis, which involves the joining together of ends of the intestine after a section has been removed.
* People with a history of blood clots in the blood vessels (thromboembolism).
* Heart failure.
* People who have recently had a heart attack.
* High blood pressure (hypertension).
* Diabetes, or a family history of diabetes.
* Underactive thyroid gland (hypothyroidism).
* Epilepsy.
* Glaucoma, or a family history of glaucoma.
* Current severe psychiatric illness, or a personal or family history of psychiatric illness, including depression, manic depression or schizophrenia.
* History of psychiatric illness caused by the use of a corticosteroid.
* Osteoporosis.
* Women who have passed the menopause.
* Abnormal muscle weakness (myasthenia gravis).
* People who have previously experienced muscle disorders (myopathy) caused by steroids.
* People with a history of tuberculosis (TB).
* Herpes simplex virus infection of the eye.
* People with a low level of potassium in their blood (hypokalaemia).
Not to be used in
* People with widespread infection, unless this is being treated with specific anti-infectives.
* Corticosteroids should not be used for the management of head injury or stroke because they are unlikely to be of benefit and may even be harmful.
* Betnesol injection should not be injected directly into tendons.
This medicine should not be used if you are allergic to one or any of its ingredients. Please inform your doctor or pharmacist if you have previously experienced such an allergy.
If you feel you have experienced an allergic reaction, stop using this medicine and inform your doctor or pharmacist immediately.
Pregnancy and breastfeeding
Certain medicines should not be used during pregnancy or breastfeeding. However, other medicines may be safely used in pregnancy or breastfeeding providing the benefits to the mother outweigh the risks to the unborn baby. Always inform your doctor if you are pregnant or planning a pregnancy, before using any medicine.
* When administered for long periods or repeatedly during pregnancy, corticosteroids may increase the risk of slowed growth in the developing baby. They may also cause the baby to make less of its own steroid hormones after birth, but this usually resolves on its own and rarely causes any problems. When used during pregnancy betamethasone may also temporarily reduce the baby’s heart rate and body movements. As a result this medicine should be used with caution during pregnancy, and only if the expected benefit to the mother is greater than any possible risk to the developing baby. Seek further medical advice from your doctor.
* This medicine passes into breast milk. It should be used with caution in mothers who are breastfeeding and only if the benefits to the mother outweigh any risks to the nursing infant. Lower doses taken by the mother are unlikely to significantly affect the baby, but if the mother is taking high doses for long periods of time, the medicine could cause the baby's adrenal glands to make less of their own steroid hormones. Seek medical advice from your doctor.
Side effects
Medicines and their possible side effects can affect individual people in different ways. The following are some of the side effects that are known to be associated with this medicine. Just because a side effect is stated here does not mean that all people using this medicine will experience that or any side effect.
* Raised blood sugar level.
* Increased appetite and weight gain.
* Increased susceptibility to infections and increased severity of infections (see warnings above).
* Effects on the gut, such as indigestion or abdominal bloating, nausea, ulceration in the stomach or intestine, inflammation of the pancreas (pancreatitis).
* Ulceration or thrush infection in the throat.
* Muscle weakness or wasting.
* Thinning of the bones (osteoporosis) and increased risk of breaking a bone.
* Effects on the skin, such as skin thinning, impaired healing, acne, bruising, stretch marks, increased sweating, change in pigmentation, increased hair growth (hirsutism).
* Psychiatric reactions, such as mood changes (including irritability, depression and suicidal thoughts), psychotic reactions (including mania, delusions and hallucinations), anxiety, confusion, memory loss, sleep disturbances (see warning above).
* Cushing's syndrome, characterised by a moon face.
* Menstrual disturbances.
* Decrease in the production of natural steroids by the adrenal glands (adrenal suppression - see warning above).
* Effects on the eyes, such as raised pressure inside the eye (glaucoma), cataracts.
* Slowed growth in children and adolescents.
* Hiccups.
* Blood clots in the blood vessels (thromboembolism).
The side effects listed above may not include all of the side effects reported by the medicine's manufacturer.
For more information about any other possible risks associated with this medicine, please read the information provided with the medicine or consult your doctor or pharmacist.
How can this medicine affect other medicines?
It is important to tell your doctor or pharmacist what medicines you are already taking, including those bought without a prescription and herbal medicines, before you start treatment with this medicine. Similarly, check with your doctor or pharmacist before taking any new medicines while being treated with this one, to ensure that the combination is safe.
Betamethasone may increase blood sugar levels and so may oppose the blood sugar lowering effects of antidiabetic medicines. People with diabetes may need an increase in their dose of insulin or antidiabetic tablets.
Betamethasone may enhance the anti-blood-clotting effect of anticoagulant medicines such as warfarin. People taking anticoagulant medicines in combination with betamethasone should have their blood clotting time (INR) regularly monitored, particularly after starting or stopping treatment with betamethasone and after any dose changes.
If betamethasone is used in combination with non-steroidal anti-inflammatory drugs (NSAIDs) eg ibuprofen, there may be an increased risk of side effects on the gut, such as stomach ulceration and bleeding.
Betamethasone may decrease the blood levels of salicylates such as aspirin. When betamethasone is stopped, this may result in excessive levels of the salicylate, unless the dose is readjusted.
The following medicines may increase the removal of betamethasone from the body, thus reducing its effects. You may need a larger dose of betamethasone if you are also taking any of these medicines:
* barbituates, eg amobarbital, phenobarbital
* carbamazepine
* phenytoin
* primidone
* rifabutin
* rifampicin.
The effect of corticosteroids may be reduced in the three to four days following use of mifepristone.
The following medicines may reduce the removal of betamethasone from the body and so may increase its effects or side effects:
* ciclosporin (betamethasone may also increase the blood level and risk of side effects of ciclosporin)
* itraconazole
* ketoconazole
* macrolide-type antibiotics, eg erythromycin
* protease inhibitors, eg ritonavir.
Betamethasone may decrease the body's immune response. This means that vaccines may be less effective if given during treatment, because the body does not produce sufficient antibodies. Live vaccines may cause serious infections. Live vaccines include: measles, mumps, rubella, MMR, BCG, chickenpox, oral polio, oral typhoid and yellow fever. These should not be given to people whose immune system is underactive due to treatment with this medicine.
Corticosteroids can cause fluid and salt retention and so may oppose the effects of antihypertensive medicines used to treat high blood pressure, and diuretics such as furosemide. However, betamethasone is much less likely than other corticosteroids to have this effect.
Corticosteroids can also lower the amount of potassium in the blood, though this is much less likely with betamethasone than with other corticosteroids. However, there may be an increased chance of the level of potassium in the blood falling too low (hypokalaemia) if betamethasone is used in combination with the following medicines:
* acetazolamide
* amphotericin
* beta agonists, eg salbutamol, salmeterol, terbutaline
* carbenoxolone
* potassium-losing diuretics, eg furosemide, bendroflumethiazide
* theophylline.
Other medicines containing the same active ingredient
Betamethasone has many different uses and comes in many different forms. The factsheets below contain information about betamethasone used in various areas of the body.
-----------------------
Steroid Injection for Fetal Lung Development
Injections of corticosteroids for fetal lung development has been praised as one of the best advances in fetal medicine in the 90s. Since 1994 the National Institutes for Health and other professional organizations have encouraged their use in promoting the development of fetal lung development in moms who were at risk for preterm labor or birth.
Betamethasone and dexamethasone are the two most commonly used steroids. The average protocol was to give to intramuscular injections (IM) 24 hours apart. Some practitioners also choose to continually repeat the dosages every week until the birth. The injections had to be given 24-48 hours prior to the birth for maximum effect. They were also best used between weeks 24 and 34 gestation.
The use of the steroids provided benefits for the lung development in the premature infants to reduce the risk of respiratory distress syndrome (RDS) as well as to reduce the risk of intracranial hemorrhaging and some other potential benefits.
However, recent studies say that the benefits of multiple doses is questionable, particularly in light of potential risks. Citing the "limited quality" of the studies of multiple doses and the potential disadvantages the National Institute of Health issued a statement of August 18th that a single dose was sufficient in achieving the benefits desired.
Potential down sides to multiple doses can include: psychomotor delays, behavioral problems and the fact that the effects on neonatal mortality aren't known between the single and multiple dose courses. In separate findings by an Israeli study it was also noted that there is an increase in maternal infection with the use of steroids, so limiting doses may help with this side effect as well.
The steroid injection is to help mature the baby's lungs in case of premature delivery. Yes it has potential side effects (EVERY medication has potential side effects...there's no free ride when it comes to pharmacology). It develops the fetal lungs early because it sets up a very stressful environment for the baby. Decreased birth weight, decreased brain size, abnormal brain development, adverse effects on the fetal immune system, are just some of the potential side effects. Steroid injections for fetal lung development should not be taken lightly. It should be used only for cases where premature delivery is expected and the potential benefits outweigh the potential side effects.
I don't know why the doc told her that one injection is harmful but more than one is not. Sounds like she didn't really understand what was being explained to her.
http://www.naturallycurly.com/curltalk/showthread.php?t=27953
Antenatal corticosteroids for fetal lung development
Examples
betamethasone Celestone Soluspan dexamethasone Dalalone Decadron
How It Works
Betamethasone and dexamethasone cause an immature fetus's lungs to produce a compound called surfactant. A full-term baby's lungs naturally produce surfactant, which lubricates the lining of the air sacs within the lungs. This allows the inner surfaces of the air sacs to slide against one another without sticking during breathing. Premature infants whose lungs have begun producing surfactant have an improved ability to breathe on their own, or with less respiratory treatment, after birth.
When preterm birth between 24 and 34 weeks of pregnancy (gestation) is expected within 7 days, betamethasone or dexamethasone is given to the mother in order to affect the fetus. Betamethasone is given in 2 injections, 24 hours apart. Dexamethasone is given every 12 hours for 4 doses.
If delivery does not occur within 7 days of treatment, the injections should not be repeated. Recent guidelines issued by the National Institutes of Health discourage such repeat courses of treatment, based on concerns about fetal harm from repeat treatments.1
Why It Is Used
Corticosteroids are considered standard treatment for women who are 24 to 34 weeks pregnant and may deliver within the next 1 to 7 days, with or without preterm premature rupture of membranes (pPROM).1
Betamethasone and dexamethasone are corticosteroids, also called glucocorticoids, that are given before birth (antenatally) to speed up a preterm fetus's lung development. Either is used when a mother is in preterm labor and birth may occur in 24 to 48 hours. This helps prevent the occurrence of respiratory distress syndrome (RDS) and related complications following premature birth.
Many infants born at 33 to 34 weeks' gestation have sufficient lung maturity to breathe on their own. However, considering the low-risk, high-benefit nature of this treatment, corticosteroids are typically used up to 34 weeks of pregnancy.
WebMD
Betamethasone is often used in patients with premature labor at about 26-34 weeks' gestation to stimulate fetal lung maturation The benefits of this therapy are: Reduction in incidence of respiratory distress syndrome (RDS) Decreased severity of RDS if it occurs Decreased incidence of, and mortality from, intracranial hemorrhage Increased survival of premature infants Betamethasone crosses the placenta to the fetus . The drug is partially metabolized (47%) by the perfused placenta to its inactive 11-ketosteroid derivative, but less so than other corticosteroids, although the differences are not statistically significant .
In patients with premature rupture of the membranes (PROM), administration of betamethasone to the mother does not always reduce the frequency of RDS or perinatal mortality . An increased risk of maternal infection has also been observed in patients with PROM treated with corticosteroids . In a study comparing betamethasone therapy with nonsteroid management of women with PROM, neonatal sepsis was observed in 23% (5 of 22) of steroid-exposed newborns vs. only 2% (1 of 46) of the non-steroid-exposed group . A 1985 study also found increased neonatal sepsis in exposed newborns who were delivered more than 48 hours after PROM, 18.6% (14 of 75) vs. 7.4% (4 of 54) of nonexposed controls . In addition, moderate to severe respiratory morbidity was increased over that in controls, 21.3% vs. 11.1%, as well as overall mortality, 8% vs. 1.8% . Other reports, however, have noted beneficial effects of betamethasone administration to patients with PROM with no increase in infectious morbidity (15,23,24,). In women colonized with group B streptococci, the combined use of betamethasone and ampicillin improved the outcome of preterm pregnancies with PROM .
Betamethasone therapy is less effective in decreasing the incidence of RDS in male infants than in female infants . The reasons for this difference have not been discovered. Slower lung maturation in male fetuses has been cited as a major contributing factor to the sex differential noted in neonatal mortality. Therapy is also less effective in multiple pregnancies , even when doses have been doubled . In twins, only the first-born seems to benefit from antenatal steroid therapy .
An increased incidence of hypoglycemia in newborns exposed in utero to betamethasone has been reported . Other investigators have not observed this effect.
In the initial study examining the effect of betamethasone on RDS, investigators reported an increased risk of fetal death in patients with severe preeclampsia. They proposed that the corticosteroid had an adverse effect on placentas already damaged by vascular disease. A second study did not confirm these findings .
A case of suspected betamethasone-induced leukemoid reaction was observed in an 880-g, 30-weeks'-gestation female infant whose mother received 12 mg of betamethasone 4 hours prior to delivery . A second case, in a female infant born at 25-26 weeks' 71 hours after betamethasone, was published in 1997 . Within about 710 days, the white blood cell count had returned to normal in both infants. A 1984 study examined the effect of betamethasone on leukocyte counts in mothers with PROM or premature labor . No effect, as compared to untreated controls, was found in either group.
A case of acute, life-threatening exacerbation of muscular weakness requiring intubation and mechanical ventilation was reported in a 24-year-old woman who was treated with betamethasone, 12 mg IM, to enhance fetal lung maturity at 32 weeks' gestation . The onset of symptoms occurred 30 minutes after the corticosteroid dose. The authors attributed the crisis to betamethasone (adrenocorticosteroids are known to aggravate myasthenia) after other potential causes were ruled out. The infant was delivered by emergency cesarean section and, except for the typical problems related to prematurity, he had a normal hospital course.
Hypertensive crisis associated with the use of ritodrine and betamethasone has been reported . Systolic blood pressure was above 300 mm Hg with a diastolic pressure of 120 mm Hg. Although the hypertension was probably caused by ritodrine, it is not known whether the corticosteroid was a contributing factor.
Breast Feeding Summary
No reports describing the use of betamethasone during human lactation have been located. The molecular weight (about 435 for the acetate salt and about 517 for the sodium phosphate salt) are low enough, however, that excretion into milk should be expected.
http://drugsafetysite.com/betamethasone/
What should I watch for while taking betamethasone?
Visit your prescriber or health care professional for regular checks on your progress. If you are using corticosteroids for a long time, carry an identification card with your name, the type and dose of corticosteroid, and your prescriber's name and address. Do not suddenly stop using betamethasone. You may need to gradually reduce the dose, so that your body can adjust. Follow the advice of your prescriber or health care professional.
If you receive corticosteroids for a long time, avoid contact with people who have an infection. You may be at an increased risk from infection while receiving betamethasone. Tell your prescriber or health care professional if you are exposed to anyone with measles or chickenpox, or if you develop sores or blisters that do no heal properly.
People who are taking certain dosages of betamethasone may need to avoid immunization with certain vaccines or may need to have changes in their vaccination schedules to ensure adequate protection from certain diseases. Make sure to tell your prescriber or health care professional that you are taking betamethasone before receiving any vaccine.
If you are diabetic, betamethasone can affect your blood sugar levels. Check with your prescriber or health care professional if you need help adjusting the dose of your diabetic medicine.
If you are receiving betamethasone injections every day, you may need to watch your diet. Your body can also lose potassium while you receive this medicine. Ask your prescriber or health care professional about your diet, especially about your salt intake.
If you are going to have surgery tell your prescriber or health care professional that you are receiving betamethasone, or have taken it within the last 12 months.
If betamethasone has been injected into one of your joints, do not put too much stress on the joint for a while. Talk to your prescriber or health care professional about how much you can use the joint while it is healing.
Elderly patients have an increased risk of side effects from betamethasone.
Betamethasone can interfere with certain lab tests and can cause false skin test results.
What side effects may I notice from receiving betamethasone?
Side effects that you should report to your prescriber or health care professional as soon as possible:
• bloody or black, tarry stools
• confusion, excitement, restlessness, a false sense of well-being
• eye pain, decreased or blurred vision, or bulging eyes
• fever, sore throat, sneezing, cough, or other signs of infection
• frequent passing of urine
• hallucinations (seeing and hearing things that are not really there)
• increased thirst
• irregular heartbeat
• menstrual problems
• mental depression, mood swings, mistaken feelings of self-importance, mistaken feelings of being mistreated
• muscle cramps or muscle weakness
• nausea, vomiting
• pain in hips, back, ribs, arms, shoulders, or legs
• pain, redness, inflammation or scarring at the injection site
• rounding out of face
• skin problems, acne
• stomach pain
• swelling of feet or lower legs
• thin or shiny skin at the injection site
• unusual bruising or red pinpoint spots on the skin
• unusual tiredness or weakness
• weight gain or weight loss
• wounds that will not heal
Side effects that usually do not require medical attention (report to your prescriber or health care professional if they continue or are bothersome):
• headache
• increased appetite
• increased sweating
• nervousness, restlessness, or difficulty sleeping
• unusual increased growth of hair on the face or body
http://www.answers.com/topic/betamethasone-injection
Betamethasone is a corticosteroids, and as such can cause the following side effects:
Increased thirst and urination, lethargy, increased appetite, abortion during pregnancy, immune suppression (and thus more susceptible to other illnesses), muscle weakness and possible atrophy, stomach ulcers, diarrhea, panting, and possible bone weakness.
Now, keep in mind, these side effects are often rare, except for the increased drinking, urinating and eating. Also, these are much more likely to be seen in long term use, not one injection.
Read more: http://www.justanswer.com/questions/
Tuesday, June 1, 2010
Diet in gestational diabetes:
Some tips from experts regarding eating well during pregnancy with gestational diabetes.
How should I eat during my pregnancy?
As with any pregnancy, it is important to eat the proper foods to meet the nutritional needs of the mother and fetus. An additional goal for women with gestational diabetes is to maintain a proper diet to keep blood sugars as normal as possible.
Protein Equivalents
The daily need for calories increases by 300 calories during the second and third trimesters of pregnancy. If non pregnant calorie intake was 1800 calories per day and weight gain was maintained, a calorie intake of 2100 calories per day is usual from 14 weeks until delivery. This is the equivalent of an additional 8 ounce glass of 2% milk and onehalf of a sandwich (1 slice of bread, approximately 1 ounce of meat, and I teaspoon of margarine, mayonnaise, etc.) per day. The need for protein also increases during pregnancy. Make sure your diet includes foods high in protein, but not high in fat . Most vitamins and minerals are also needed in larger amounts during pregnancy. This can be attained by increasing dairy products, especially those low in fat, and making sure you include whole grain cereals and breads, as well as fruits and vegetables in your diet each day. To make sure you get enough folate (a B vitamin critical during pregnancy) and iron, your obstetrician will probably recommend a prenatal vitamin. Prenatal vitamins do not replace a good diet; they merely help you to get the nutrients you need. To absorb the most iron from your prenatal vitamin, take it at night before going to bed, or in the morning on an empty stomach.
The Daily Food Guide serves as a guideline for food sources that provide important vitamins and minerals, as well as carbohydrates, protein, and fiber during pregnancy. The recommended minimal servings per day appear in parenthesis after each food group listed. This guide emphasizes foods that are low in fat and in sugar
Daily Food Guide(Each item equals one serving)
Milk and Milk Products
(4 Servings Per Day)
cup milk, skim or low-fat
(high protein calcium, Vitamin D)
1/3 cup powdered non-fat milk
1 cup reconstituted powdered non fat-milk
1-1/2 oz Low-fat cheese
Meat, Poultry, Fish, and Meat Substitutes
(5-6 Servings Per Day)
oz.Cooked poultry, fish, or lean meat (beef,lamb,pork) (high protein B, vitamins, iron)
1 tbsp.peanut butter
1 egg
1/4 cup low-fat cottage cheese
1/2 cup cooked dried beans or lentils
Breads, Cereals, and Other Starches
(5-6 Servings Per Day)
slice whole grain bread
(high complex carbohydrates)
(emphasize whole grams, or use fortified or enriched)
(a good source of protein, B-vitamins, fiber and minerals)
5 crackers
1 muffin,biscuit,pancake or waffle
3/4 cup dry cereal, unsweetened
1/2 cup pasta (macaroni, spaghetti), rice, mashed potatoes, or cooked cereal
1/3 cup sweet potatoes or yams
1/2 cup cooked dried beans or lentils
1/2 bagel, 1/2 English muffin, or 1/2 flour tortilla
1 small baked potato
2 taco shells
Fruit 1/2 cup
(2 Serving per day)
fruit
(fresh fruit provides fiber)
(include one vitamine C source daily)
1/2 banana, or 1 medium-sized fruit (apple, orange)
1/2 cup, orange, grapefruit, or other juice fortified with vitamine C
1/2 cup-sized grapefruite
1 cup strawberries
1/2 cup fresh apricots, nectarines, purple plums, cantaloupe or 4 halves dried apricots (vitamine A source)
Vegetables ***
(2 Serving per day)
/2 cup cooked or 1 cup raw: broccoli, spinach, carrots (vitamin A source) (include good vitamin A sources at least every other day)
1/3 cup mixed vegetables
Fats
1 tsp. butter or margarine
1 tsp. oil or mayonnaise
1 tbsp. regular salad drressing
2 tbsp. low-calorie salad dressing
1/4 cup nuts or seeds
*1 oz. lowfat cheese can also be used as 1 serving from the Meat, Poultry, Fish, and Meat Substitutes group if sufficient calcium is already being provided from 4 servings.
**This refers to plain yogurt. Commercially fruited yogurt contains a lot of added sugar
***Starchy vegetables such as corn, peas, and potatoes are included in Breads, Cereals, and Other Starches list.
The food guide is divided into six groups: milk and milk products; meat, poultry, fish, and meat substitutes; breads, cereals, and other starches; fruits; vegetables; and fats. Each group provides its own combination of vitamins, minerals, and other nutrients which play an important part in nutrition during pregnancy. Omitting the foods from one group will leave your diet inadequate in other nutrients. Plan your meals using a variety of foods within each food group, in the amounts recommended, and you'll be most likely to get all the vitamins, minerals, and other nutrients the fetus needs for growth and development.
Other Nutritional and NonNutritional Considerations:
Alcohol
There is no known safe level of alcohol to allow during pregnancy. Daily heavy alcohol intake causes severe defects in development of the body and brain of the fetus, called Fetal Alcohol Syndrome. Even moderate drinking is associated with delayed fetal growth, spontaneous abortions, and lowered birth weight in babies. The Surgeon General's office warns: “Women who are pregnant or even considering pregnancy should avoid alcohol completely and should be aware of the alcohol content of food and drugs.”
Salt
Salt restriction is no longer routinely advised during pregnancy. Recent research shows that during pregnancy the body needs salt to help provide the proper fluid balance. Your health care provider may recommend that you use salt in moderation.
Caffeine
Studies conflict on the potential danger of caffeine to the fetus. Caffeine is found primarily in coffee, tea, and some sodas (Table 6). Moderation is recommended. Talk to your doctor or other health professional about the maximum amount of caffeine recommended.
Megavitamins
Megavitamins are defined as 10 times the Recommended Dietary Allowance* of vitamins and minerals and are not recommended for pregnant women. Although it is possible to get all of the necessary nutrients from food alone, your doctor may prescribe some prenatal vitamins and minerals. If taken regularly, along with a balanced diet, you will be getting all the vitamins and minerals needed during your pregnancy.
Smoking
Research has shown without question that smoking during pregnancy increases the risk of fetal death and pre-term delivery, impairs fetal growth, and can lead to low birth weight. It is best to stop smoking entirely and permanently, or at the very least, to cut back drastically on the number of cigarettes you smoke.
What food patterns help keep blood sugar levels normal?
The following outlines food patterns which help to keep blood sugar levels within an acceptable range.
Avoid sugar and foods high in sugar. Most women with gestational diabetes, just like those without diabetes, have a desire for something sweet in their diet. In pregnant women, sugar is rapidly absorbed into the blood and requires a larger release of insulin to maintain normal blood sugar levels. Without the larger release of insulin, blood sugar levels will increase excessively when you eat sugar-containing foods.
There are many forms of sugar such as table sugar, honey, brown sugar, corn syrup, maple syrup, turbinado sugar, high fructose corn syrup, and molasses. Generally, food that ends in “ose” is a sugar (e.g., sucrose, dextrose, and glucose).
Foods that usually contain high amounts of sugar include pies, cakes, cookies, ice cream, candy, soft drinks, fruit drinks, fruit packed in syrup, commercially fruited yogurt, jams, jelly, doughnuts, and sweet rolls. Many of these foods are high in fat as well.
Be sure to check the list of ingredients on food products. Ingredients are listed in order of amount. If an ingredient is first on the list, it is present in the highest amount. If some type of sugar is listed first, second, or third on the list of ingredients, the product should be avoided. If sugar is further down, fourth, fifth, or sixth, it probably will not cause your blood sugar levels to go up excessively.
Fruit juices should only be taken with a meal and limited to 6 ounces. Tomato juice is a good choice because it is low in sugar. Six ounces of most other juice (apple, grapefruit, orange) with no sugar added still contain approximately 4 to 5 teaspoons of sugar. However, these do not contain much of the fiber of a piece of fruit which normally would act to slow the absorption of sugar into the blood. If you drink juice frequently to quench your thirst during the day, a high blood sugar level may result. Use only whole fruit for snacks.
To help with the occasional sweet tooth that we all have, artificial sweeteners may be used in foods. Aspartame has been extensively tested for safety. Use during pregnancy has been approved by the Food and Drug Administration and by the American Medical Association's Review Board. However, aspartame has not been tested for longterm safety and has not been on the market very long. It may be best to avoid its use until more tests have been done.
Saccharin is not advised during pregnancy. Likewise, use of mannitol, xylitol, sorbitol, or other artificial sweeteners is not recommended until further research is done.
Fructose is a special type of sugar that is slowly absorbed into the system. A small amount of fructose can be used if your blood sugar levels are within normal range. However, fructose still has 4 calories per gram, as much as table sugar. High fructose corn syrup is part fructose and part corn syrup, making it very similar to table sugar in composition. It will raise blood sugar levels and should definitely be avoided.
*Dietary allowances established by the National Academy of Sciences-National Research Council.
Emphasize the use of complex carbohydrates. These include vegetables, cereal, grains, beans, peas, and other starchy foods. A wellbalanced diet with plenty of fiber provided by vegetables, dried beans, cereals, and other starchy foods decreases the amount of insulin your body needs to keep blood sugars within a normal range. Anything that decreases the need for insulin is beneficial The American Diabetes Association recommends that at least one-half of your calories come from complex carbohydrates. Starchy foods include pasta, rice, grains, cereals, crackers, bread, potatoes, dried beans, peas, and legumes. Also, contrary to popular belief, carbohydrates are not highly fattening when eaten in moderate amounts and without the rich sauces and toppings often added.
Emphasize foods high in dietary fiber. Fiber is the edible portion of foods of plant origin that is not digested (e.g., skins, membranes, seeds, bran). Foods with a high fiber content include whole grain cereals and breads, fruits, vegetables, and legumes (dried peas and beans). Fiber aids digestion and helps prevent constipation. The fiber found in fruits, vegetables, and legumes also helps keep your blood sugar level from becoming too high without requiring extra insulin.
Keep your diet low in fat. Some fat is needed to help with the absorption of certain vitamins and to provide the essential fatty acids necessary for fetal growth. A diet which is high in fat causes the insulin to react in a less efficient manner, necessitating more insulin to keep blood sugar levels within normal range. Foods high in saturated fats such as fatty meats, butter, bacon, cream (light, coffee, sour cream, etc.), and whole milk cheeses are likely to be high in total fat. Most foods with saturated fat are also high in cholesterol because they are fats from animal origin. However, foods such as crackers made with coconut, palm, or palm kernel oil can be high in saturated fats as well. Read labels carefully. Unsaturated fats are found in foods such as fish, margarine and vegetable oils. Keep your use of salad dressings to a minimum and whenever possible use those prepared with olive oil. To help keep the diet lower in fat, avoid adding extra fats such as rich sauces and creamy desserts, and bake or broil foods instead of frying them. Replacing fatty foods with those high in complex carbohydrates is also helpful.
Include a bedtime snack that is a good source of protein and complex carbohydrates.
Women with gestational diabetes have a tendency toward lower than normal blood sugar levels during the night. This causes the body to increase its utilization of fats as a fuel source. As fat is used, ketones (discussed later) are produced as a byproduct of the breakdown of fats, and in large amounts, may be harmful to the fetus. This can be prevented by having a bedtime snack that provides protein and complex carbohydrates such as starchy foods. Starch will stabilize your blood sugar level in the early night, while protein acts as a longacting stabilizer.
Examples of a bedtime snack are:
1 oz. Americanprocessed cheese + 5 crackers
1/2 chicken sandwich on whole wheat bread
3 cups unbuttered popcorn + 1/4 cup nuts
If you need to take insulin, a bedtime snack is critical and you should not omit it. When taken by injection, insulin acts to lower blood sugar level, even during the night when meals are not eaten. A bedtime snack is protective against low blood sugars while sleeping or upon arising. If a bedtime snack causes heartburn, sleep with your head raised on pillows, and be careful that you are not eating too large a bedtime snack.
How do I plan meals?
A registered dietitian or qualified nutritionist can help you plan a meal pattern that is right for you. Most women with gestational diabetes need three meals and a bedtime snack each day. It is unwise for anyone who is pregnant to go long periods of time (greater than 5 hours) without eating, as this will produce ketones. Extra snacks are necessary if your schedule results in a long time between meals. Blood sugars will be easier to keep in the normal range if meal times and amounts (total calories) are evenly spaced. It's more likely that a higher blood sugar will result if the majority of calories are eaten at dinner than if they are distributed more evenly throughout the day. If insulin injections prove necessary, the time at which meals are eaten and the amounts eaten should be approximately the same from day to day. Do not skip meals and snacks, as this often results in hypoglycemia (low blood sugar), which may be harmful to the fetus and makes you feel irritable, shaky, or may result in a headache.
Sample Menu — 2000 Calories
This diet is planned for women whose normal non-pregnant weight should be 130135 lbs. For women who weigh less than 130 before pregnancy, the diet should contain fewer calories. Women who are overweight are at higher risk for gestational diabetes. Your health care provider can discuss this and help you make necessary changes
What can be done to slow weight gain during pregnancy?
Gaining too much weight during pregnancy will make blood sugar levels higher than normal for women with gestational diabetes. Yet, for many pregnant women it is very difficult to gain weight slowly and still get all of the recommended nutrients. Luckily, fat, which is high in calories (9 calories per gram), is needed in only small amounts during pregnancy. Carbohydrates and protein, in contrast to fat, provide only 4 calories per gram. To cut calories without depriving the fetus of any necessary nutritional factors, it is best to avoid fats and fatty foods.
· Avoid highfat meats. Choose lean cuts of beef, pork, and lamb. Emphasize more fish and poultry (without the skin).
· Avoid frying meat, fish, or poultry in added oil, shortening, or lard. Bake, broil, or roast instead.
· Avoid foods fried in oil such as chips, french fries, and doughnuts. Substitute pretzels, unbuttered popcorn, or breadsticks instead.
· Avoid using cream sauces and butter sauces, as well as salt pork for seasoning on vegetables. Season with herbs instead.
· Avoid using the fat drippings from meat or poultry for gravy. Use broth or bouillon instead and thicken with cornstarch.
· Avoid using mayonnaise or oil for salads. Use vinegar, lemon juice, or low-calorie salad dressings instead.
To help reduce calories choose low-fat dairy products. During pregnancy you need 1200 mg calcium daily to build the fetal skeleton without drawing from maternal calcium stores. Table 7 points out foods in which the calcium content is almost the same, yet the calories are not due to the difference in fat content.
The difference between 600 calories and 340 calories is only 260 calories and may seem insignificant. Yet, if your diet is cut by 260 calories daily for 1 week, your weight gain slows down by approximately 1/2 pound per week. In other words, instead of gaining 1-1/2 pounds per week you will only gain 1 pound per week.
If cheese is a part of your daily diet, use lowfat cheeses such as lowfat cottage cheese, Neufchatel, mozzarella, farmers, and pot cheese. Avoid using cream cheese, as it has little protein and most of its calories come from fat.
Even though pregnancy can be a very hectic time, with little time for meal preparation, eat less and less often at “fast food” restaurants. Studies have shown that some foods from fast food restaurants average 40 to 60 percent of their calories from fat, and are quite high in calories.* For example, chicken and fish that are coated with batter and deep-fried in fat may contain more fat and calories than a hamburger or roast beef sandwich.
*Fast Food Facts: Nutritive and Exchange Values for Fast Food Restaurants Marion J. Franz, International Diabetes Center. Minneapolis, Minnesota, 1987. 54 pp.
Go lightly when using butter and margarine. Adding only an extra three pats of butter or margarine (same calories) daily could add an extra pound of weight gain next month. It may be better to emphasize the use of foods rich in complex carbohydrates that don't use butter, margarine, or cream sauce to make them palatable. Many people find rice, noodles, and spaghetti tasty without a lot of butter. Use a variety of spices and herbs (such as curry, garlic, and parsley) to flavor rice and tomato sauce to flavor pasta without additional fats.
It is also a good idea to eat small amounts frequently, thereby keeping the edge off your appetite. This will assist your “self-control” in avoiding large portions of food that you should not have. Avoid skipping meals or trying to cut back drastically on breakfast or lunch. It will leave you too hungry for the next meal to exercise any control. Your doctor or dietitian can help you determine how you can cut extra calories.
You may find it helpful to keep food records of what you eat, as most of us tend to forget or not realize the extent of our snacking. Recording everything you eat or drink tends to be a sobering and instructive experience.
Be careful to maintain a weight gain of at least 1/2 pound per week, over several weeks, if you are in the second trimester (14 weeks or more of gestation). Cutting back more than this may increase the risk of having a low-birth-weight infant.
http://www.childbirthsolutions.com/articles/pregnancy/gestationaldiet/index.php
How should I eat during my pregnancy?
As with any pregnancy, it is important to eat the proper foods to meet the nutritional needs of the mother and fetus. An additional goal for women with gestational diabetes is to maintain a proper diet to keep blood sugars as normal as possible.
Protein Equivalents
| Food | Grams of Protein |
| 1 cup milk | 8 |
| 1 cup plain nonfat yogurt | 8 |
| 1 ounce American processed cheese | 7 |
| 1 ounce low-fat cheese | 7 |
| 1 tbsp. peanut butter | 7 |
| 1/4 cup cottage cheese | 7 |
| 1/2 cup cooked dried beans | 7 |
| 1 slice whole wheat bread | 3 |
| 1/2 cup flaked cereal bran or corn | 3 |
The daily need for calories increases by 300 calories during the second and third trimesters of pregnancy. If non pregnant calorie intake was 1800 calories per day and weight gain was maintained, a calorie intake of 2100 calories per day is usual from 14 weeks until delivery. This is the equivalent of an additional 8 ounce glass of 2% milk and onehalf of a sandwich (1 slice of bread, approximately 1 ounce of meat, and I teaspoon of margarine, mayonnaise, etc.) per day. The need for protein also increases during pregnancy. Make sure your diet includes foods high in protein, but not high in fat . Most vitamins and minerals are also needed in larger amounts during pregnancy. This can be attained by increasing dairy products, especially those low in fat, and making sure you include whole grain cereals and breads, as well as fruits and vegetables in your diet each day. To make sure you get enough folate (a B vitamin critical during pregnancy) and iron, your obstetrician will probably recommend a prenatal vitamin. Prenatal vitamins do not replace a good diet; they merely help you to get the nutrients you need. To absorb the most iron from your prenatal vitamin, take it at night before going to bed, or in the morning on an empty stomach.
The Daily Food Guide serves as a guideline for food sources that provide important vitamins and minerals, as well as carbohydrates, protein, and fiber during pregnancy. The recommended minimal servings per day appear in parenthesis after each food group listed. This guide emphasizes foods that are low in fat and in sugar
Daily Food Guide(Each item equals one serving)
Milk and Milk Products
(4 Servings Per Day)
cup milk, skim or low-fat
(high protein calcium, Vitamin D)
1/3 cup powdered non-fat milk
1 cup reconstituted powdered non fat-milk
1-1/2 oz Low-fat cheese
Meat, Poultry, Fish, and Meat Substitutes
(5-6 Servings Per Day)
oz.Cooked poultry, fish, or lean meat (beef,lamb,pork) (high protein B, vitamins, iron)
1 tbsp.peanut butter
1 egg
1/4 cup low-fat cottage cheese
1/2 cup cooked dried beans or lentils
Breads, Cereals, and Other Starches
(5-6 Servings Per Day)
slice whole grain bread
(high complex carbohydrates)
(emphasize whole grams, or use fortified or enriched)
(a good source of protein, B-vitamins, fiber and minerals)
5 crackers
1 muffin,biscuit,pancake or waffle
3/4 cup dry cereal, unsweetened
1/2 cup pasta (macaroni, spaghetti), rice, mashed potatoes, or cooked cereal
1/3 cup sweet potatoes or yams
1/2 cup cooked dried beans or lentils
1/2 bagel, 1/2 English muffin, or 1/2 flour tortilla
1 small baked potato
2 taco shells
Fruit 1/2 cup
(2 Serving per day)
fruit
(fresh fruit provides fiber)
(include one vitamine C source daily)
1/2 banana, or 1 medium-sized fruit (apple, orange)
1/2 cup, orange, grapefruit, or other juice fortified with vitamine C
1/2 cup-sized grapefruite
1 cup strawberries
1/2 cup fresh apricots, nectarines, purple plums, cantaloupe or 4 halves dried apricots (vitamine A source)
Vegetables ***
(2 Serving per day)
/2 cup cooked or 1 cup raw: broccoli, spinach, carrots (vitamin A source) (include good vitamin A sources at least every other day)
1/3 cup mixed vegetables
Fats
1 tsp. butter or margarine
1 tsp. oil or mayonnaise
1 tbsp. regular salad drressing
2 tbsp. low-calorie salad dressing
1/4 cup nuts or seeds
*1 oz. lowfat cheese can also be used as 1 serving from the Meat, Poultry, Fish, and Meat Substitutes group if sufficient calcium is already being provided from 4 servings.
**This refers to plain yogurt. Commercially fruited yogurt contains a lot of added sugar
***Starchy vegetables such as corn, peas, and potatoes are included in Breads, Cereals, and Other Starches list.
The food guide is divided into six groups: milk and milk products; meat, poultry, fish, and meat substitutes; breads, cereals, and other starches; fruits; vegetables; and fats. Each group provides its own combination of vitamins, minerals, and other nutrients which play an important part in nutrition during pregnancy. Omitting the foods from one group will leave your diet inadequate in other nutrients. Plan your meals using a variety of foods within each food group, in the amounts recommended, and you'll be most likely to get all the vitamins, minerals, and other nutrients the fetus needs for growth and development.
Other Nutritional and NonNutritional Considerations:
Alcohol
There is no known safe level of alcohol to allow during pregnancy. Daily heavy alcohol intake causes severe defects in development of the body and brain of the fetus, called Fetal Alcohol Syndrome. Even moderate drinking is associated with delayed fetal growth, spontaneous abortions, and lowered birth weight in babies. The Surgeon General's office warns: “Women who are pregnant or even considering pregnancy should avoid alcohol completely and should be aware of the alcohol content of food and drugs.”
Salt
Salt restriction is no longer routinely advised during pregnancy. Recent research shows that during pregnancy the body needs salt to help provide the proper fluid balance. Your health care provider may recommend that you use salt in moderation.
Caffeine
Studies conflict on the potential danger of caffeine to the fetus. Caffeine is found primarily in coffee, tea, and some sodas (Table 6). Moderation is recommended. Talk to your doctor or other health professional about the maximum amount of caffeine recommended.
Caffeine Comparisons
| Food | Serving | Amount of Caffeine |
| Regular coffee | 8 oz | 80-200ma |
| Instant coffee | 8 oz | 60-100 ma |
| Decaffeinated coffee | 8 oz | 3-5 ma |
| Tea | 8 oz | 60-65 ma |
| Carbonated drinks | | |
| e.g. colas | 12 oz | 30-65 mg |
| Hot chocolate | 8 oz | 13 ma |
Megavitamins
Megavitamins are defined as 10 times the Recommended Dietary Allowance* of vitamins and minerals and are not recommended for pregnant women. Although it is possible to get all of the necessary nutrients from food alone, your doctor may prescribe some prenatal vitamins and minerals. If taken regularly, along with a balanced diet, you will be getting all the vitamins and minerals needed during your pregnancy.
Smoking
Research has shown without question that smoking during pregnancy increases the risk of fetal death and pre-term delivery, impairs fetal growth, and can lead to low birth weight. It is best to stop smoking entirely and permanently, or at the very least, to cut back drastically on the number of cigarettes you smoke.
What food patterns help keep blood sugar levels normal?
The following outlines food patterns which help to keep blood sugar levels within an acceptable range.
Avoid sugar and foods high in sugar. Most women with gestational diabetes, just like those without diabetes, have a desire for something sweet in their diet. In pregnant women, sugar is rapidly absorbed into the blood and requires a larger release of insulin to maintain normal blood sugar levels. Without the larger release of insulin, blood sugar levels will increase excessively when you eat sugar-containing foods.
There are many forms of sugar such as table sugar, honey, brown sugar, corn syrup, maple syrup, turbinado sugar, high fructose corn syrup, and molasses. Generally, food that ends in “ose” is a sugar (e.g., sucrose, dextrose, and glucose).
Foods that usually contain high amounts of sugar include pies, cakes, cookies, ice cream, candy, soft drinks, fruit drinks, fruit packed in syrup, commercially fruited yogurt, jams, jelly, doughnuts, and sweet rolls. Many of these foods are high in fat as well.
Be sure to check the list of ingredients on food products. Ingredients are listed in order of amount. If an ingredient is first on the list, it is present in the highest amount. If some type of sugar is listed first, second, or third on the list of ingredients, the product should be avoided. If sugar is further down, fourth, fifth, or sixth, it probably will not cause your blood sugar levels to go up excessively.
Fruit juices should only be taken with a meal and limited to 6 ounces. Tomato juice is a good choice because it is low in sugar. Six ounces of most other juice (apple, grapefruit, orange) with no sugar added still contain approximately 4 to 5 teaspoons of sugar. However, these do not contain much of the fiber of a piece of fruit which normally would act to slow the absorption of sugar into the blood. If you drink juice frequently to quench your thirst during the day, a high blood sugar level may result. Use only whole fruit for snacks.
To help with the occasional sweet tooth that we all have, artificial sweeteners may be used in foods. Aspartame has been extensively tested for safety. Use during pregnancy has been approved by the Food and Drug Administration and by the American Medical Association's Review Board. However, aspartame has not been tested for longterm safety and has not been on the market very long. It may be best to avoid its use until more tests have been done.
Saccharin is not advised during pregnancy. Likewise, use of mannitol, xylitol, sorbitol, or other artificial sweeteners is not recommended until further research is done.
Fructose is a special type of sugar that is slowly absorbed into the system. A small amount of fructose can be used if your blood sugar levels are within normal range. However, fructose still has 4 calories per gram, as much as table sugar. High fructose corn syrup is part fructose and part corn syrup, making it very similar to table sugar in composition. It will raise blood sugar levels and should definitely be avoided.
*Dietary allowances established by the National Academy of Sciences-National Research Council.
Emphasize the use of complex carbohydrates. These include vegetables, cereal, grains, beans, peas, and other starchy foods. A wellbalanced diet with plenty of fiber provided by vegetables, dried beans, cereals, and other starchy foods decreases the amount of insulin your body needs to keep blood sugars within a normal range. Anything that decreases the need for insulin is beneficial The American Diabetes Association recommends that at least one-half of your calories come from complex carbohydrates. Starchy foods include pasta, rice, grains, cereals, crackers, bread, potatoes, dried beans, peas, and legumes. Also, contrary to popular belief, carbohydrates are not highly fattening when eaten in moderate amounts and without the rich sauces and toppings often added.
Emphasize foods high in dietary fiber. Fiber is the edible portion of foods of plant origin that is not digested (e.g., skins, membranes, seeds, bran). Foods with a high fiber content include whole grain cereals and breads, fruits, vegetables, and legumes (dried peas and beans). Fiber aids digestion and helps prevent constipation. The fiber found in fruits, vegetables, and legumes also helps keep your blood sugar level from becoming too high without requiring extra insulin.
Keep your diet low in fat. Some fat is needed to help with the absorption of certain vitamins and to provide the essential fatty acids necessary for fetal growth. A diet which is high in fat causes the insulin to react in a less efficient manner, necessitating more insulin to keep blood sugar levels within normal range. Foods high in saturated fats such as fatty meats, butter, bacon, cream (light, coffee, sour cream, etc.), and whole milk cheeses are likely to be high in total fat. Most foods with saturated fat are also high in cholesterol because they are fats from animal origin. However, foods such as crackers made with coconut, palm, or palm kernel oil can be high in saturated fats as well. Read labels carefully. Unsaturated fats are found in foods such as fish, margarine and vegetable oils. Keep your use of salad dressings to a minimum and whenever possible use those prepared with olive oil. To help keep the diet lower in fat, avoid adding extra fats such as rich sauces and creamy desserts, and bake or broil foods instead of frying them. Replacing fatty foods with those high in complex carbohydrates is also helpful.
Include a bedtime snack that is a good source of protein and complex carbohydrates.
Women with gestational diabetes have a tendency toward lower than normal blood sugar levels during the night. This causes the body to increase its utilization of fats as a fuel source. As fat is used, ketones (discussed later) are produced as a byproduct of the breakdown of fats, and in large amounts, may be harmful to the fetus. This can be prevented by having a bedtime snack that provides protein and complex carbohydrates such as starchy foods. Starch will stabilize your blood sugar level in the early night, while protein acts as a longacting stabilizer.
Examples of a bedtime snack are:
1 oz. Americanprocessed cheese + 5 crackers
1/2 chicken sandwich on whole wheat bread
3 cups unbuttered popcorn + 1/4 cup nuts
If you need to take insulin, a bedtime snack is critical and you should not omit it. When taken by injection, insulin acts to lower blood sugar level, even during the night when meals are not eaten. A bedtime snack is protective against low blood sugars while sleeping or upon arising. If a bedtime snack causes heartburn, sleep with your head raised on pillows, and be careful that you are not eating too large a bedtime snack.
How do I plan meals?
A registered dietitian or qualified nutritionist can help you plan a meal pattern that is right for you. Most women with gestational diabetes need three meals and a bedtime snack each day. It is unwise for anyone who is pregnant to go long periods of time (greater than 5 hours) without eating, as this will produce ketones. Extra snacks are necessary if your schedule results in a long time between meals. Blood sugars will be easier to keep in the normal range if meal times and amounts (total calories) are evenly spaced. It's more likely that a higher blood sugar will result if the majority of calories are eaten at dinner than if they are distributed more evenly throughout the day. If insulin injections prove necessary, the time at which meals are eaten and the amounts eaten should be approximately the same from day to day. Do not skip meals and snacks, as this often results in hypoglycemia (low blood sugar), which may be harmful to the fetus and makes you feel irritable, shaky, or may result in a headache.
Sample Menu — 2000 Calories
This diet is planned for women whose normal non-pregnant weight should be 130135 lbs. For women who weigh less than 130 before pregnancy, the diet should contain fewer calories. Women who are overweight are at higher risk for gestational diabetes. Your health care provider can discuss this and help you make necessary changes
What can be done to slow weight gain during pregnancy?
Gaining too much weight during pregnancy will make blood sugar levels higher than normal for women with gestational diabetes. Yet, for many pregnant women it is very difficult to gain weight slowly and still get all of the recommended nutrients. Luckily, fat, which is high in calories (9 calories per gram), is needed in only small amounts during pregnancy. Carbohydrates and protein, in contrast to fat, provide only 4 calories per gram. To cut calories without depriving the fetus of any necessary nutritional factors, it is best to avoid fats and fatty foods.
· Avoid highfat meats. Choose lean cuts of beef, pork, and lamb. Emphasize more fish and poultry (without the skin).
· Avoid frying meat, fish, or poultry in added oil, shortening, or lard. Bake, broil, or roast instead.
· Avoid foods fried in oil such as chips, french fries, and doughnuts. Substitute pretzels, unbuttered popcorn, or breadsticks instead.
· Avoid using cream sauces and butter sauces, as well as salt pork for seasoning on vegetables. Season with herbs instead.
· Avoid using the fat drippings from meat or poultry for gravy. Use broth or bouillon instead and thicken with cornstarch.
· Avoid using mayonnaise or oil for salads. Use vinegar, lemon juice, or low-calorie salad dressings instead.
To help reduce calories choose low-fat dairy products. During pregnancy you need 1200 mg calcium daily to build the fetal skeleton without drawing from maternal calcium stores. Table 7 points out foods in which the calcium content is almost the same, yet the calories are not due to the difference in fat content.
The difference between 600 calories and 340 calories is only 260 calories and may seem insignificant. Yet, if your diet is cut by 260 calories daily for 1 week, your weight gain slows down by approximately 1/2 pound per week. In other words, instead of gaining 1-1/2 pounds per week you will only gain 1 pound per week.
If cheese is a part of your daily diet, use lowfat cheeses such as lowfat cottage cheese, Neufchatel, mozzarella, farmers, and pot cheese. Avoid using cream cheese, as it has little protein and most of its calories come from fat.
Even though pregnancy can be a very hectic time, with little time for meal preparation, eat less and less often at “fast food” restaurants. Studies have shown that some foods from fast food restaurants average 40 to 60 percent of their calories from fat, and are quite high in calories.* For example, chicken and fish that are coated with batter and deep-fried in fat may contain more fat and calories than a hamburger or roast beef sandwich.
*Fast Food Facts: Nutritive and Exchange Values for Fast Food Restaurants Marion J. Franz, International Diabetes Center. Minneapolis, Minnesota, 1987. 54 pp.
Go lightly when using butter and margarine. Adding only an extra three pats of butter or margarine (same calories) daily could add an extra pound of weight gain next month. It may be better to emphasize the use of foods rich in complex carbohydrates that don't use butter, margarine, or cream sauce to make them palatable. Many people find rice, noodles, and spaghetti tasty without a lot of butter. Use a variety of spices and herbs (such as curry, garlic, and parsley) to flavor rice and tomato sauce to flavor pasta without additional fats.
It is also a good idea to eat small amounts frequently, thereby keeping the edge off your appetite. This will assist your “self-control” in avoiding large portions of food that you should not have. Avoid skipping meals or trying to cut back drastically on breakfast or lunch. It will leave you too hungry for the next meal to exercise any control. Your doctor or dietitian can help you determine how you can cut extra calories.
You may find it helpful to keep food records of what you eat, as most of us tend to forget or not realize the extent of our snacking. Recording everything you eat or drink tends to be a sobering and instructive experience.
Be careful to maintain a weight gain of at least 1/2 pound per week, over several weeks, if you are in the second trimester (14 weeks or more of gestation). Cutting back more than this may increase the risk of having a low-birth-weight infant.
http://www.childbirthsolutions.com/articles/pregnancy/gestationaldiet/index.php
Gestational diabetes and weight gain:
Mom has become a little tensed after she found out today that there has been a decrease in weight by approx 1kg.
The main thing is she is maintaining a proper diet control and doing regular exercises due to gestational diabetes.
Is it due to this that she is gradually losing part of her weight?.. who knows!
Dr. will be able to judge this better.
Actually Dr. Vidya Desai, mom's gynecologist explained to her that she has even seen many patients gaining total of 5kgs during her pregnancy and has delivered healthy 3kg babies. Hence in gestational diabetes weight gain calculations is done little differently. No need to worry as long as my growth and weight gain is ok. But it is very difficult for mom to understand how much of weight is gained and me and how how much she is losing due to diet control . Mom give me a weighing scale ..i want to measure my weights here inside you and tell you every week :)
Lets see what experts have to say regarding weight gain for gestational diabetic moms..
How much weight should I gain?
Of all questions asked by pregnant women, this is the most common. The answer is particularly important for women with gestational diabetes. The weight that you gain is a rough indication of how much nutrition is available to the fetus for growth. An inadequate weight gain may result in a small baby who lacks protective calorie reserves at birth. This baby may have more illness during the first year of life. An excessive weight gain during pregnancy, however, has an insulinresistant effect, just like the hormones produced by the placenta, and will make your blood sugar level higher.
The “optimal” weight to gain depends on the weight that you are before becoming pregnant. Your pre-pregnancy weight is also a rough indication of how well-nourished you are before becoming pregnant. If you are at a desirable weight for your body size before you become pregnant, a weight gain of 24 to 27 pounds is recommended. If you are approximately 20 pounds or more above your desirable weight before pregnancy, a weight gain of 24 pounds is recommended. Many overweight women, however, have healthy babies and gain only 20 pounds. If you become pregnant when you are underweight, you need to gain more weight during the pregnancy to give your baby the extra nutrition he or she needs for the first year. You should gain 28 to 36 pounds, depending on how underweight you are before becoming pregnant. Table 3 shows whether your pre-pregnancy weight is considered underweight, normal weight, or overweight. Your nutrition advisor or health care provider can recommend an appropriate weight gain. How your weight gain is distributed is illustrated here.
PrePregnancy Weight
*Normal weight for “thin-boned” women will be closer to the lower end of this range. For “big-boned” women, it will be closer to the higher end.
Total recommended weight gain is often not as helpful as a weekly rate of gain. Most women gain 3 to 5 pounds during the first trimester (first 3 months) of pregnancy. During the second and third trimesters, a good rate of weight gain is about threequarters of a pound to one pound per week. Gaining too much weight (2 or more pounds per week) results in putting on too much body fat. This extra body fat produces an insulin-resistant effect which requires the body to produce more insulin to keep blood sugar levels normal. An inability to produce more insulin, as in gestational diabetes, causes your blood sugar levels to rise above acceptable levels. If weight gain has been excessive, often limiting weight gain to approximately three-quarters of a pound per week (3 pounds per month) can return blood sugar levels to normal. Fetal growth and development depend on proper nourishment and will be placed at risk by drastically reducing calories. However, you can limit weight gain by cutting back on excessive calories and by eating a nutritionally-sound diet that meets your needs and the needs of your baby.
Remember that dieting and severely cutting back on weight gain may increase the risk of delivering prematurely. If blood sugar levels continue to go up and you are not gaining excessive weight or eating improperly, the safest therapy for the well-being of the fetus is insulin.
Occasionally, your weight may go up rapidly in the last trimester (after 28 weeks) and you may notice an increase in water retention, such as swelling in the feet, fingers, and face. If there is any question as to whether the rapid weight gain is due to eating too many calories or too much water retention, keeping records of how much food you eat and your exercise patterns at this time will be very helpful. In addition, by examining your legs and body for signs of fluid retention, your physician can help you to determine the cause of your weight gain. If your weight gain is due to water retention, cutting back drastically on calories may actually cause more fluid retention. Bed rest and resting on your side will help you to lose the build-up of fluid. Limit your intake of salt (sodium chloride) and very salty foods, as they tend to contribute to water retention.
Marked fluid retention when combined with an increase in blood pressure and possibly protein in the urine are the symptoms of pre-eclampsia. This is a disorder of pregnancy that can be harmful to both the mother and baby. Inform your obstetrician of any rapid weight gain, especially if you are eating moderately and gaining more than 2 pounds per week. Should you develop pre-eclampsia, be especially careful to eat a well-balanced diet with adequate calories.
After being diagnosed as having gestational diabetes, many women notice a slower weight gain as they start cutting the various sources of sugar out of their diet. This seems to be harmless and lasts only 1 or 2 weeks. It may be that sweets were contributing a substantial amount of calories to the diet.
http://www.childbirthsolutions.com/articles/pregnancy/gestationaldiet/index.php
The main thing is she is maintaining a proper diet control and doing regular exercises due to gestational diabetes.
Is it due to this that she is gradually losing part of her weight?.. who knows!
Dr. will be able to judge this better.
Actually Dr. Vidya Desai, mom's gynecologist explained to her that she has even seen many patients gaining total of 5kgs during her pregnancy and has delivered healthy 3kg babies. Hence in gestational diabetes weight gain calculations is done little differently. No need to worry as long as my growth and weight gain is ok. But it is very difficult for mom to understand how much of weight is gained and me and how how much she is losing due to diet control . Mom give me a weighing scale ..i want to measure my weights here inside you and tell you every week :)
Lets see what experts have to say regarding weight gain for gestational diabetic moms..
How much weight should I gain?
Of all questions asked by pregnant women, this is the most common. The answer is particularly important for women with gestational diabetes. The weight that you gain is a rough indication of how much nutrition is available to the fetus for growth. An inadequate weight gain may result in a small baby who lacks protective calorie reserves at birth. This baby may have more illness during the first year of life. An excessive weight gain during pregnancy, however, has an insulinresistant effect, just like the hormones produced by the placenta, and will make your blood sugar level higher.
The “optimal” weight to gain depends on the weight that you are before becoming pregnant. Your pre-pregnancy weight is also a rough indication of how well-nourished you are before becoming pregnant. If you are at a desirable weight for your body size before you become pregnant, a weight gain of 24 to 27 pounds is recommended. If you are approximately 20 pounds or more above your desirable weight before pregnancy, a weight gain of 24 pounds is recommended. Many overweight women, however, have healthy babies and gain only 20 pounds. If you become pregnant when you are underweight, you need to gain more weight during the pregnancy to give your baby the extra nutrition he or she needs for the first year. You should gain 28 to 36 pounds, depending on how underweight you are before becoming pregnant. Table 3 shows whether your pre-pregnancy weight is considered underweight, normal weight, or overweight. Your nutrition advisor or health care provider can recommend an appropriate weight gain. How your weight gain is distributed is illustrated here.
PrePregnancy Weight
Use this chart to determine if your prepregnancy weight is normal, underweight, or overweight.
| Heigth without shoes | Underweight if you weighed this or less | Normal weight *Range | Overweight if you weight this or more |
| 4'10" | 88 | 89-108 | 109 |
| 4'11" | 91 | 92-112 | 113 |
| 5' | 94 | 95-115 | 116 |
| 5'1" | 99 | 100-121 | 122 |
| 5'2" | 104 | 105-127 | 128 |
| 5'3" | 108 | 109-132 | 133 |
| 5'4" | 113 | 114-138 | 139 |
| 5'5" | 118 | 119-144 | 145 |
| 5'6" | 123 | 124-150 | 151 |
| 5'7" | 127 | 128-155 | 156 |
| 5'8" | 132 | 133-161 | 162 |
| 5'9" | 137 | 138-167 | 168 |
| 5'10" | 142 | 143-173 | 174 |
| 5'11" | 146 | 147-178 | 179 |
| 6' | 151 | 152-184 | 185 |
*Normal weight for “thin-boned” women will be closer to the lower end of this range. For “big-boned” women, it will be closer to the higher end.
Total recommended weight gain is often not as helpful as a weekly rate of gain. Most women gain 3 to 5 pounds during the first trimester (first 3 months) of pregnancy. During the second and third trimesters, a good rate of weight gain is about threequarters of a pound to one pound per week. Gaining too much weight (2 or more pounds per week) results in putting on too much body fat. This extra body fat produces an insulin-resistant effect which requires the body to produce more insulin to keep blood sugar levels normal. An inability to produce more insulin, as in gestational diabetes, causes your blood sugar levels to rise above acceptable levels. If weight gain has been excessive, often limiting weight gain to approximately three-quarters of a pound per week (3 pounds per month) can return blood sugar levels to normal. Fetal growth and development depend on proper nourishment and will be placed at risk by drastically reducing calories. However, you can limit weight gain by cutting back on excessive calories and by eating a nutritionally-sound diet that meets your needs and the needs of your baby.
Remember that dieting and severely cutting back on weight gain may increase the risk of delivering prematurely. If blood sugar levels continue to go up and you are not gaining excessive weight or eating improperly, the safest therapy for the well-being of the fetus is insulin.
Occasionally, your weight may go up rapidly in the last trimester (after 28 weeks) and you may notice an increase in water retention, such as swelling in the feet, fingers, and face. If there is any question as to whether the rapid weight gain is due to eating too many calories or too much water retention, keeping records of how much food you eat and your exercise patterns at this time will be very helpful. In addition, by examining your legs and body for signs of fluid retention, your physician can help you to determine the cause of your weight gain. If your weight gain is due to water retention, cutting back drastically on calories may actually cause more fluid retention. Bed rest and resting on your side will help you to lose the build-up of fluid. Limit your intake of salt (sodium chloride) and very salty foods, as they tend to contribute to water retention.
Marked fluid retention when combined with an increase in blood pressure and possibly protein in the urine are the symptoms of pre-eclampsia. This is a disorder of pregnancy that can be harmful to both the mother and baby. Inform your obstetrician of any rapid weight gain, especially if you are eating moderately and gaining more than 2 pounds per week. Should you develop pre-eclampsia, be especially careful to eat a well-balanced diet with adequate calories.
After being diagnosed as having gestational diabetes, many women notice a slower weight gain as they start cutting the various sources of sugar out of their diet. This seems to be harmless and lasts only 1 or 2 weeks. It may be that sweets were contributing a substantial amount of calories to the diet.
http://www.childbirthsolutions.com/articles/pregnancy/gestationaldiet/index.php
Subscribe to:
Posts (Atom)